

Combining Multiple Types of Motor Rehabilitation Enhances Skilled Forelimb Use Following Experimental Traumatic Brain Injury in Rats
- PMID: 25761884
- PMCID: PMC5090980
- DOI: 10.1177/1545968315576577
Combining Multiple Types of Motor Rehabilitation Enhances Skilled Forelimb Use Following Experimental Traumatic Brain Injury in Rats
Abstract
Background: Neuroplasticity and neurorehabilitation have been extensively studied in animal models of stroke to guide clinical rehabilitation of stroke patients. Similar studies focused on traumatic brain injury (TBI) are lacking.
Objective: The current study was designed to examine the effects of individual and combined rehabilitative approaches, previously shown to be beneficial following stroke, in an animal model of moderate/severe TBI, the controlled cortical impact (CCI).
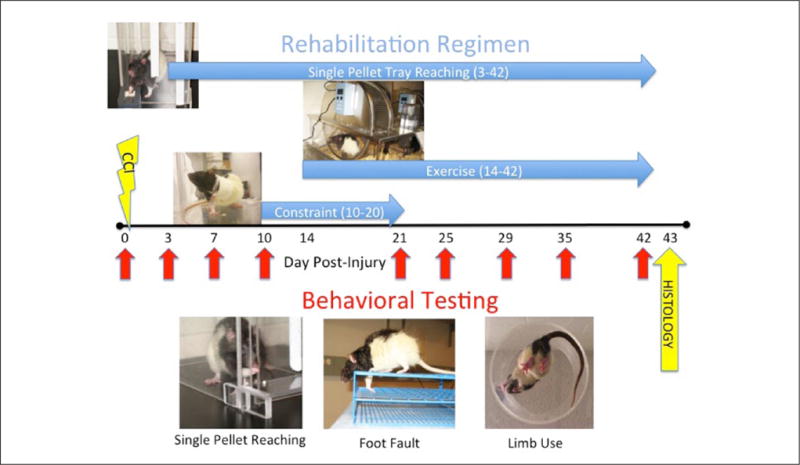
Methods: Rats received a unilateral CCI, followed by reach training, voluntary exercise, or unimpaired forelimb constraint, alone or in combination. Forelimb function was assessed at different time points post-CCI by tests of skilled reaching, motor coordination, and asymmetrical limb use.
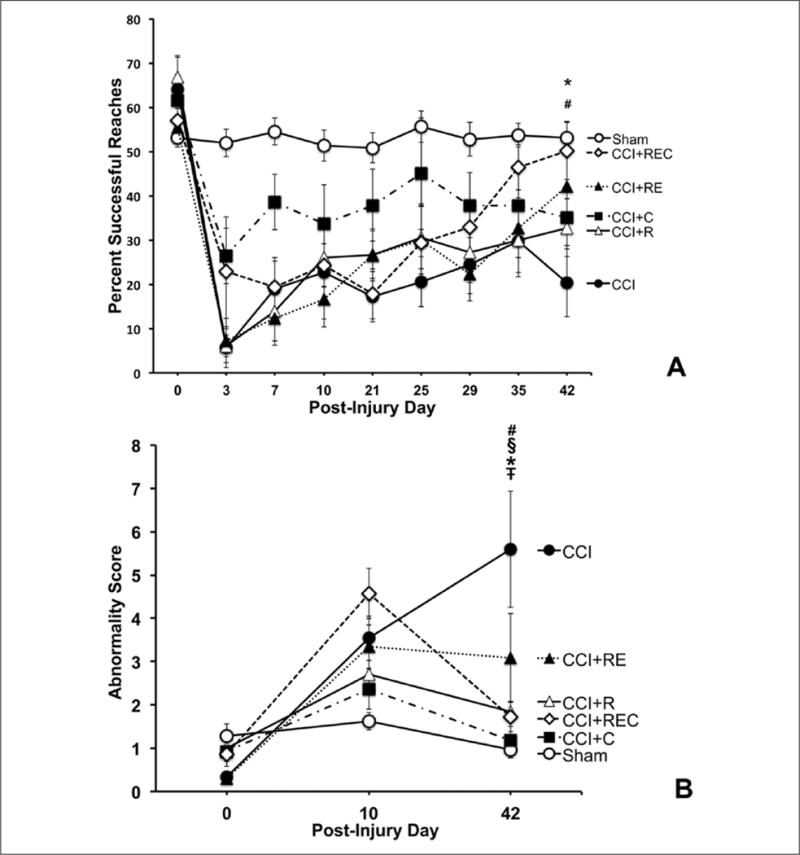
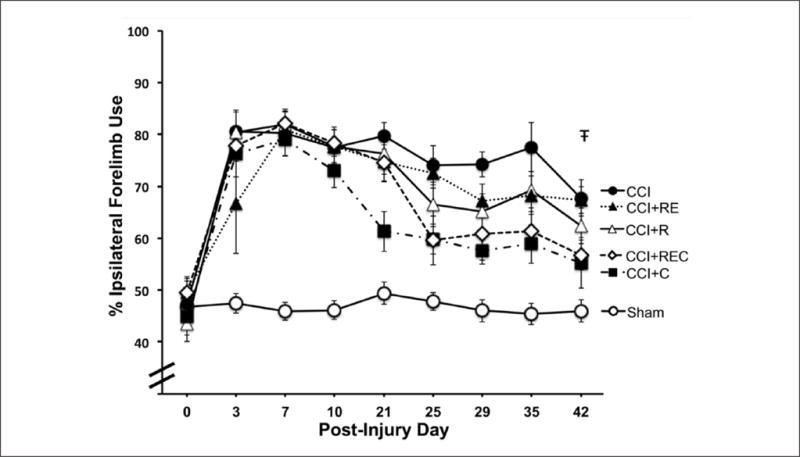
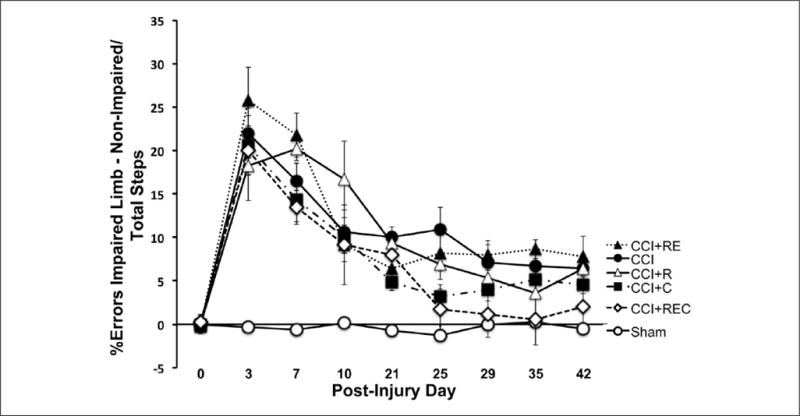
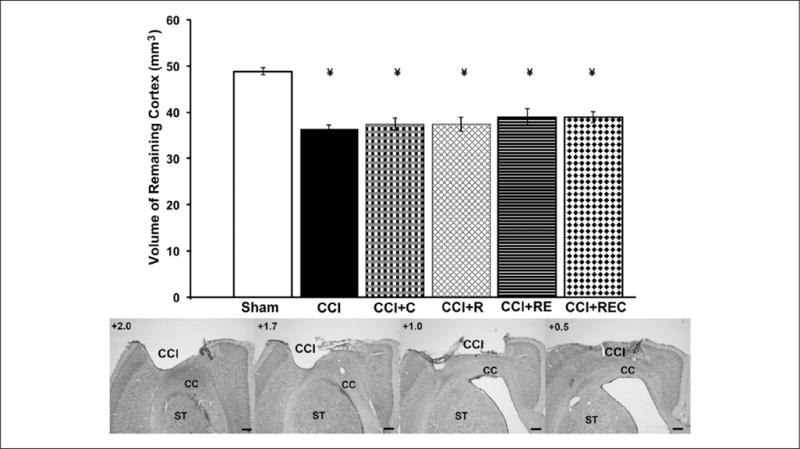
Results: Following CCI, skilled reaching and motor coordination were significantly enhanced by combinations of rehabilitation strategies, not by individual approaches. The return of symmetrical limb use benefited from forelimb constraint alone. None of the rehabilitation strategies affected the size of injury, suggesting that enhanced behavioral function was not a result of neuroprotection.
Conclusions: The current study has provided evidence that individual rehabilitation strategies shown to be beneficial in animal models of stroke are not similarly sufficient to enhance behavioral outcome in a model of TBI. Motor rehabilitation strategies for TBI patients may need to be more intense and varied. Future basic science studies exploring the underlying mechanisms of combined rehabilitation approaches in TBI as well as clinical studies comparing rehabilitation approaches for stroke versus TBI would prove fruitful.
Keywords: constraint-induced movement therapy; controlled cortical impact; exercise; motor rehabilitation; neuroplasticity; recovery of function.
© The Author(s) 2015.
Conflict of interest statement
Declaration of Conflicting Interests The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: ICMJE Uniform Disclosure Form for Potential Conflicts of Interest: Dr Kozlowski reports a grant from US Department of Defense during the conduct of the study.
Figures
References
-
- Faul M, Xu L, Wald MM, Coronado VG. Traumatic Brain Injury in the United States: Emergency Department Visits, Hospitalizations and Deaths 2002–2006. Atlanta, GA: Centers for Disease Control and Prevention; 2010.
-
- Krauss JK, Jankovic J. Movement disorders after TBI. In: Zasler ND, Katz DI, Zafonte RD, editors. Brain Injury Medicine: Principles and Practice. New York, NY: Demos; 2007. pp. 469–489.
-
- Walker WC, Pickett TC. Motor impairment after severe traumatic brain injury: a longitudinal multicenter study. J Rehabil Res Dev. 2007;44:975–982. - PubMed
-
- Kozlowski DA, Leasure JL, Schallert T. The control of movement following traumatic brain injury. Compr Physiol. 2013;3:121–139. - PubMed
-
- Weightman MM, Bolgla R, McCulloch KL, Peterson MD. Physical therapy recommendations for service members with mild traumatic brain injury. J Head Trauma Rehabil. 2010;25:206–218. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
