

Is There a Benefit to Highly Crosslinked Polyethylene in Posterior-stabilized Total Knee Arthroplasty? A Randomized Trial
- PMID: 25762016
- PMCID: PMC4686511
- DOI: 10.1007/s11999-015-4241-x
Is There a Benefit to Highly Crosslinked Polyethylene in Posterior-stabilized Total Knee Arthroplasty? A Randomized Trial
Abstract
Background: Polyethylene wear and osteolysis remain a concern with the use of modular, fixed-bearing total knee arthroplasty (TKA). A variety of highly crosslinked polyethylenes (XLPs) have been introduced to address this problem, but there are few data on the results and complications of this polyethylene in posterior-stabilized knee prostheses.
Questions/purposes: In a randomized prospective study design comparing standard polyethylene (SP) tibial inserts with XLP inserts, we asked the following questions: (1) Are there any differences in the clinical results (as measured by the classic Knee Society scoring system) and radiographic results (as measured by an evaluation for radiolucencies and osteolysis) between these groups? (2) What is the frequency of reoperation in these two groups? (3) Are there any specific complications related to XLP liners?
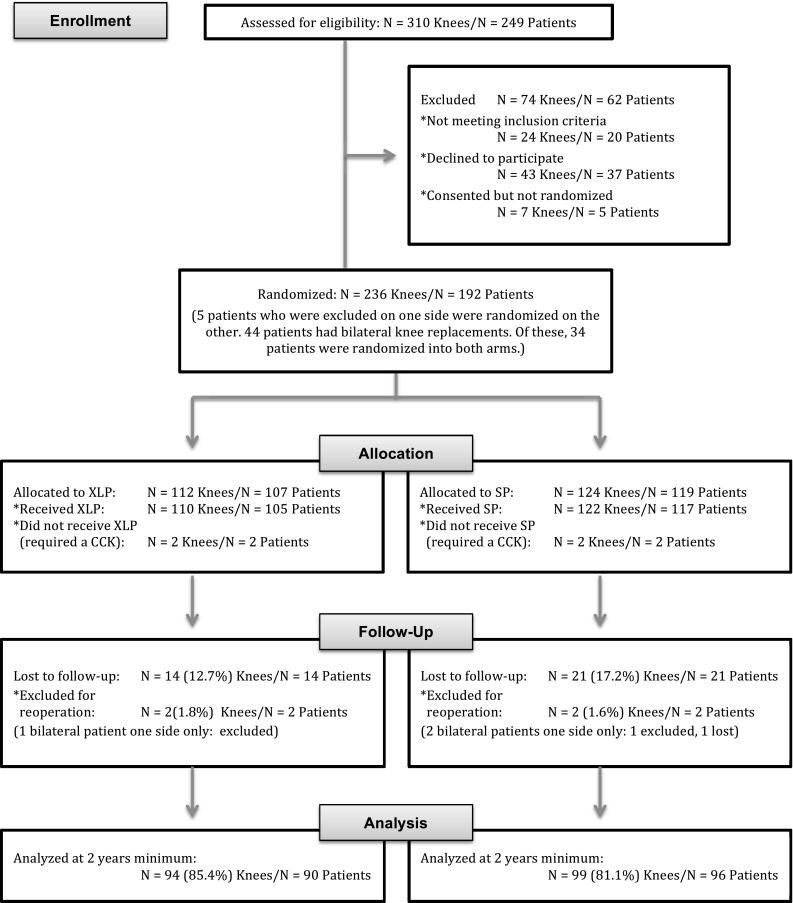
Methods: These are preliminary data from a single surgeon of a planned interim analysis of a prospective randomized study of one modular posterior-stabilized TKA. One hundred ninety-two patients (236 knees) were randomized to receive a SP compression-molded liner or a XLP (6.5 CGy electron beam-irradiated and remelted) polyethylene liner. There was no difference in the number of knees who were lost or refused followup (14 knees [13%] with XLP and 21 knees [17%] with SP). Patients were evaluated clinically using the original Knee Society scores, Lower Extremity Activity Score (LEAS), presence of knee effusion, and by standard radiographs for radiolucent lines and osteolytic lesions. This analysis was performed at a mean followup of 4.5 years (range, 2-8 years).
Results: There were no clinical differences between 99 knees with SP and 94 knees with XLP in original Knee Society total score (SP mean 95, SD 5; XLP mean 94, SD 7 [p = 0.16]); change in total score (SP mean 41, 95% confidence interval [CI], 39-41; XLP mean 43, 95% CI, 39-48 [p = 0.56]); knee function score (SP mean 64 [SD 25]; XLP mean 64 [SD 24] p = 0.98; change in function score (SP mean 22, 95% CI, 17-27; XLP mean 21, 95% CI, 17-27 [p = 0.79]); LEAS score (both SP and XLP 9 [SD 2]; p = 0.88); and change in LEAS (both SP and XLP mean 1, 95% CI, 1-2 [p = 0.0.38]). There were no differences, with the numbers available, in the presence of effusion (two of 94 XLP and five of 99 SP) with 2 years minimum followup. There were no differences in the frequency of radiolucent lines (13 knees with SP and 15 with XLP) or of osteolysis (two knees with SP and none with XLP). There was no difference in frequency of reoperation between the two groups (three infections in 110 knees allocated to the XLP group and five (two infections, one femoral loosening, one instability, one fracture plating) in 122 knees allocated to the standard group. There were no complications related to the XLP liner.
Conclusions: In this interim analysis, with the numbers available, there were no complications, but no advantages, related to the use of this XLP tibial liner. Additional enrollment has continued, and longer followup of these patients will be necessary to determine whether long-term wear characteristics differ between the groups.
Level of evidence: Level I, therapeutic study.
Figures
Similar articles
-
Prospective randomized trial of standard versus highly crosslinked tibial polyethylene in primary posterior-stabilized total knee arthroplasty: clinical and radiological follow-up at 2 to 11 years.Bone Joint J. 2019 Jul;101-B(7_Supple_C):33-39. doi: 10.1302/0301-620X.101B7.BJJ-2018-1126.R2. Bone Joint J. 2019. PMID: 31256647 Clinical Trial.
-
Highly Crosslinked-remelted versus Less-crosslinked Polyethylene in Posterior Cruciate-retaining TKAs in the Same Patients.Clin Orthop Relat Res. 2015 Nov;473(11):3588-94. doi: 10.1007/s11999-015-4425-4. Epub 2015 Jun 27. Clin Orthop Relat Res. 2015. PMID: 26115866 Free PMC article.
-
The rates of osteolysis and loosening associated with a modular posterior stabilized knee replacement. Results at five to fourteen years.J Bone Joint Surg Am. 2004 Mar;86(3):525-30. doi: 10.2106/00004623-200403000-00010. J Bone Joint Surg Am. 2004. PMID: 14996878
-
The surgical options and clinical evidence for treatment of wear or corrosion occurring with THA or TKA.Clin Orthop Relat Res. 2014 Dec;472(12):3674-86. doi: 10.1007/s11999-014-3652-4. Clin Orthop Relat Res. 2014. PMID: 25024023 Free PMC article. Review.
-
History and systematic review of wear and osteolysis outcomes for first-generation highly crosslinked polyethylene.Clin Orthop Relat Res. 2011 Aug;469(8):2262-77. doi: 10.1007/s11999-011-1872-4. Clin Orthop Relat Res. 2011. PMID: 21431461 Free PMC article.
Cited by
-
Highly cross-linked polyethylene in primary total knee arthroplasty is associated with a lower rate of revision for aseptic loosening: a meta-analysis of 962,467 cases.Arch Orthop Trauma Surg. 2022 Jun;142(6):1177-1184. doi: 10.1007/s00402-021-03887-z. Epub 2021 Apr 13. Arch Orthop Trauma Surg. 2022. PMID: 33847797 Review.
-
The Survival of Total Knee Arthroplasty: Current Data from Registries on Tribology: Review Article.HSS J. 2017 Feb;13(1):28-31. doi: 10.1007/s11420-016-9513-9. Epub 2016 Jul 15. HSS J. 2017. PMID: 28167870 Free PMC article. Review.
-
The influence of implant factors on patient outcomes in primary total knee arthroplasty.J Orthop. 2024 Jul 17;58:154-160. doi: 10.1016/j.jor.2024.07.011. eCollection 2024 Dec. J Orthop. 2024. PMID: 39157416
-
Analysis of different bicruciate-retaining tibial prosthesis design using a three dimension finite element model.Am J Transl Res. 2017 May 15;9(5):2618-2628. eCollection 2017. Am J Transl Res. 2017. PMID: 28560009 Free PMC article.
-
Comprehensive evaluation of risk factors for aseptic loosening in cemented total knee arthroplasty: A systematic review and meta-analysis.J Exp Orthop. 2024 Jul 21;11(3):e12095. doi: 10.1002/jeo2.12095. eCollection 2024 Jul. J Exp Orthop. 2024. PMID: 39035847 Free PMC article. Review.
References
-
- Berry DJ. Recognizing and identifying osteolysis around total knee arthroplasty. Instr Course Lect. 2004;440:141–148. - PubMed
-
- Bragdon CR, Doerner M, Martell J, Jarrett B, Palm H, Multicenter Study Group. Malchau H. The 2012 John Charnley Award. Clinical multicenter studies of the wear performance of highly crosslinked remelted polyethylene in THA. Clin Orthop Relat Res. 2013;471:393–402. doi: 10.1007/s11999-012-2604-0. - DOI - PMC - PubMed
-
- Ewald FC. The Knee Society total knee arthroplasty roentgenographic evaluation and scoring system. Clin Orthop Relat Res. 1989;248:9–12. - PubMed
-
- Fehring TK, Murphy JA, Hayes TD, Roberts DW, Pomeroy DL, Griffin WL. Factors influencing wear and osteolysis in press-fit condylar modular total knee replacements. Clin Orthop Relat Res. 2004;428:40–50. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
