

Two cilengitide regimens in combination with standard treatment for patients with newly diagnosed glioblastoma and unmethylated MGMT gene promoter: results of the open-label, controlled, randomized phase II CORE study
- PMID: 25762461
- PMCID: PMC4482861
- DOI: 10.1093/neuonc/nou356
Two cilengitide regimens in combination with standard treatment for patients with newly diagnosed glioblastoma and unmethylated MGMT gene promoter: results of the open-label, controlled, randomized phase II CORE study
Abstract
Background: Survival outcomes for patients with glioblastoma remain poor, particularly for patients with unmethylated O(6)-methylguanine-DNA methyltransferase (MGMT) gene promoter. This phase II, randomized, open-label, multicenter trial investigated the efficacy and safety of 2 dose regimens of the selective integrin inhibitor cilengitide combined with standard chemoradiotherapy in patients with newly diagnosed glioblastoma and an unmethylated MGMT promoter.
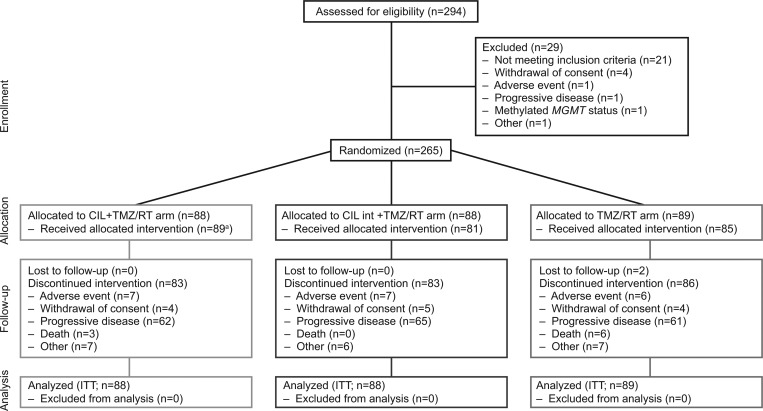
Methods: Overall, 265 patients were randomized (1:1:1) to standard cilengitide (2000 mg 2×/wk; n = 88), intensive cilengitide (2000 mg 5×/wk during wk 1-6, thereafter 2×/wk; n = 88), or a control arm (chemoradiotherapy alone; n = 89). Cilengitide was administered intravenously in combination with daily temozolomide (TMZ) and concomitant radiotherapy (RT; wk 1-6), followed by TMZ maintenance therapy (TMZ/RT→TMZ). The primary endpoint was overall survival; secondary endpoints included progression-free survival, pharmacokinetics, and safety and tolerability.
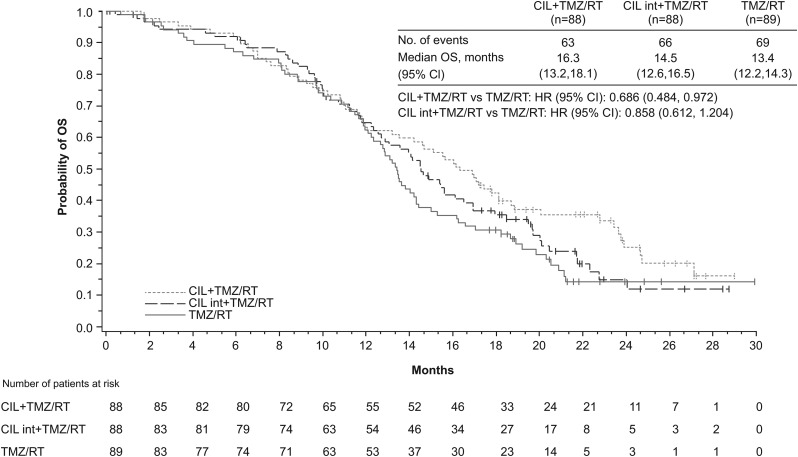
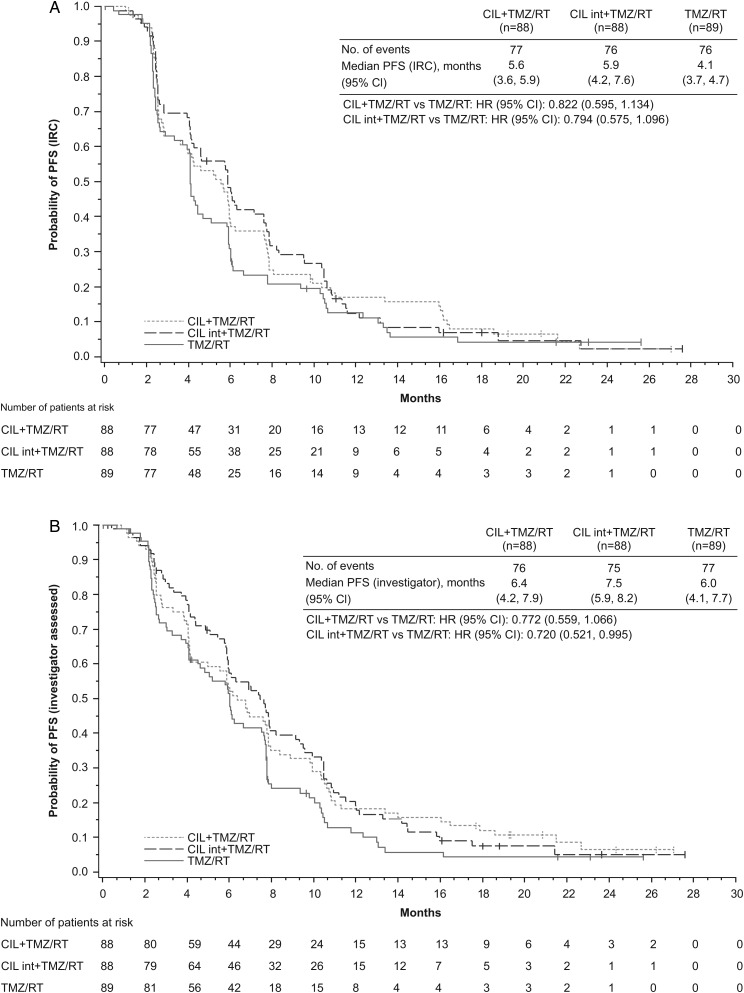
Results: Median overall survival was 16.3 months in the standard cilengitide arm (hazard ratio [HR], 0.686; 95% CI: 0.484, 0.972; P = .032) and 14.5 months in the intensive cilengitide arm (HR, 0.858; 95% CI: 0.612, 1.204; P = .3771) versus 13.4 months in the control arm. Median progression-free survival assessed per independent review committee was 5.6 months (HR, 0.822; 95% CI: 0.595, 1.134) and 5.9 months (HR, 0.794; 95% CI: 0.575, 1.096) in the standard and intensive cilengitide arms, respectively, versus 4.1 months in the control arm. Cilengitide was well tolerated.
Conclusions: Standard and intensive cilengitide dose regimens were well tolerated in combination with TMZ/RT→TMZ. Inconsistent overall survival and progression-free survival outcomes and a limited sample size did not allow firm conclusions regarding clinical efficacy in this exploratory phase II study.
Keywords: cilengitide; newly diagnosed glioblastoma; randomized phase II study; unmethylated MGMT promoter.
© The Author(s) 2015. Published by Oxford University Press on behalf of the Society for Neuro-Oncology. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Figures
Comment in
-
End of the road: confounding results of the CORE trial terminate the arduous journey of cilengitide for glioblastoma.Neuro Oncol. 2015 May;17(5):634-5. doi: 10.1093/neuonc/nov018. Epub 2015 Feb 13. Neuro Oncol. 2015. PMID: 25681307 Free PMC article. No abstract available.
References
-
- Stupp R, Mason WP, van den Bent MJ, et al. Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. N Engl J Med. 2005;352(10):987–996. - PubMed
-
- National Comprehensive Cancer Network. 2014. NCCN clinical practice guidelines in oncology (NCCN Guidelines): central nervous system cancers. Version 2.2014, Comprehensive Cancer Network, Fort Washington, PA Available at http://www.nccn.org/ Accessed March 5, 2015.
-
- Hegi ME, Diserens AC, Godard S, et al. Clinical trial substantiates the predictive value of O-6-methylguanine-DNA methyltransferase promoter methylation in glioblastoma patients treated with temozolomide. Clin Cancer Res. 2004;10(6):1871–1874. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
