

Kidney Dysfunction and Markers of Inflammation in the Multicenter AIDS Cohort Study
- PMID: 25762788
- PMCID: PMC4559190
- DOI: 10.1093/infdis/jiv159
Kidney Dysfunction and Markers of Inflammation in the Multicenter AIDS Cohort Study
Abstract
Background: Human immunodeficiency virus (HIV)-infected individuals are at higher risk for chronic kidney disease than HIV-uninfected individuals. We investigated whether the inflammation present in treated HIV infection contributes to kidney dysfunction among HIV-infected men receiving highly active antiretroviral therapy.
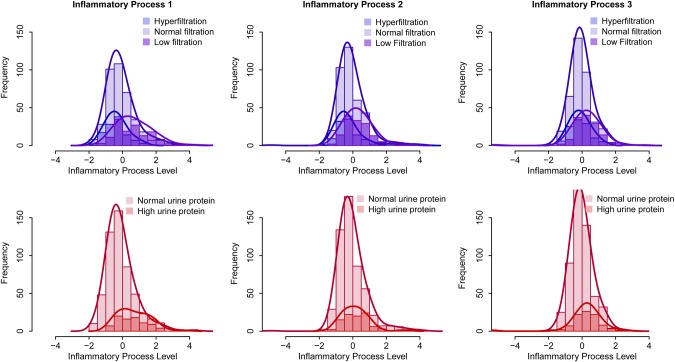
Methods: The glomerular filtration rate (GFR) was directly measured (using iohexol) along with 12 markers of inflammation in Multicenter AIDS Cohort Study participants. Exploratory factor analysis was used to identify inflammatory processes related to kidney dysfunction. The estimated levels of these inflammatory processes were used in adjusted logistic regression analyses evaluating cross-sectional associations with kidney function outcomes.
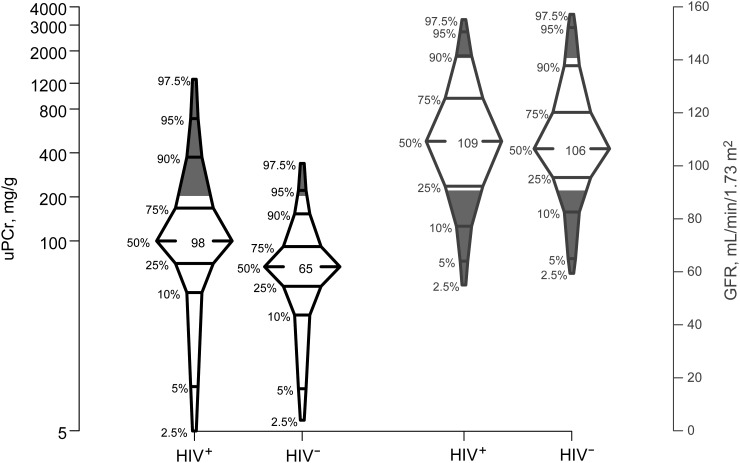
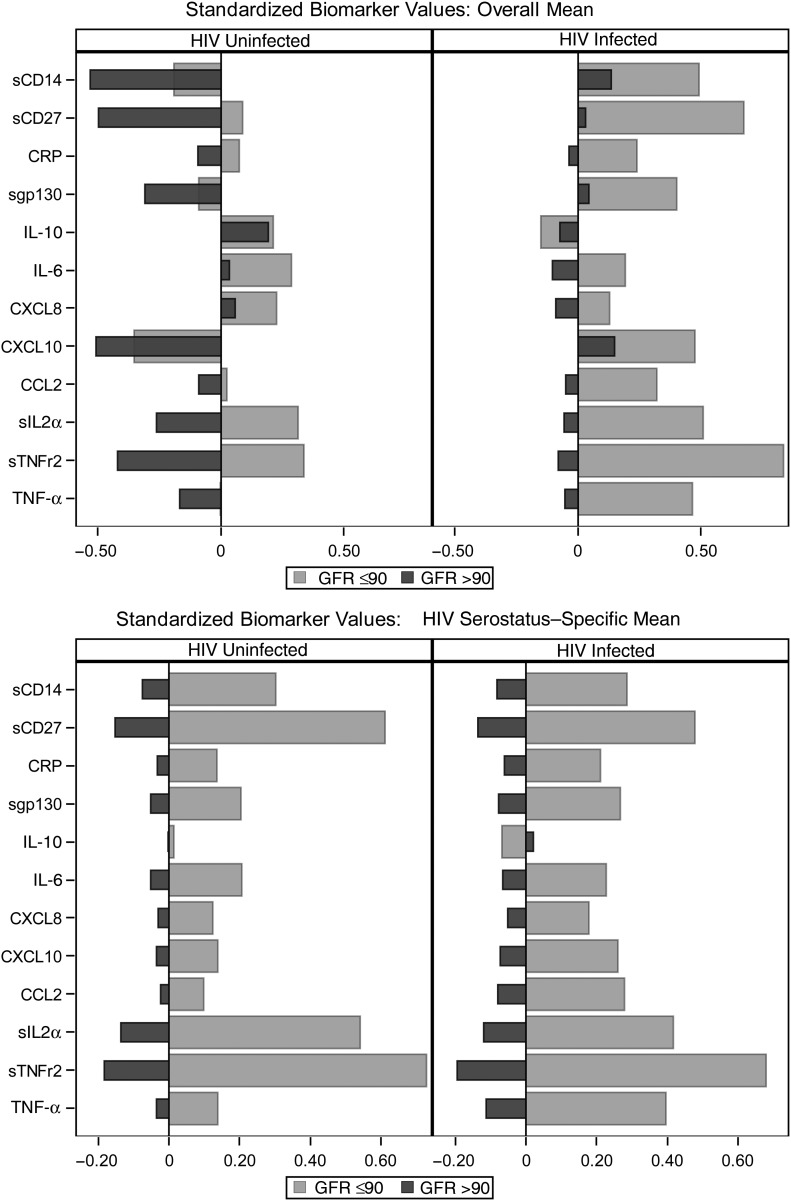
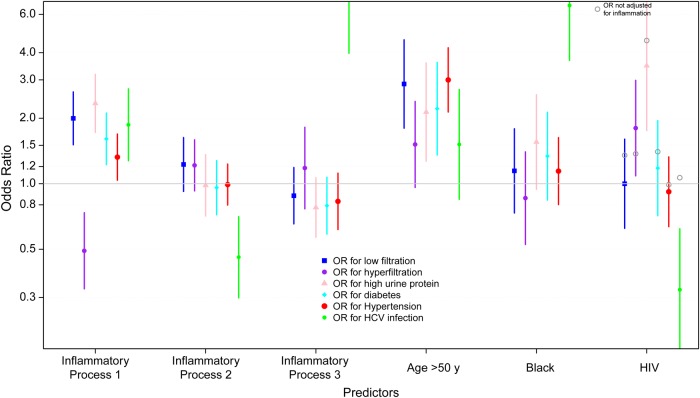
Results: There were 434 HIV-infected men receiving highly active antiretroviral therapy and 200 HIV-uninfected men. HIV-infected men were younger (median age, 51 vs 53 years) and had higher urine protein-creatinine ratios (median, 98 vs 66 mg/g) but comparable GFRs (median, 109 vs 106 mL/min|1.73 m(2)). We found an inflammatory process dominated by markers: soluble tumor necrosis factor receptor 2, soluble interleukin 2 receptor α, soluble gp130, soluble CD27, and soluble CD14. An increase of 1 standard deviation in that inflammatory process was associated with significantly greater odds of GFR ≤90 mL/min/1.73 m(2) (odds ratio, 2.0) and urine protein >200 mg/g (odds ratio, 2.3).
Conclusions: Higher circulating levels of immune activation markers among treated HIV-infected men may partially explain their higher burden of kidney dysfunction compared with uninfected men.
Keywords: HIV infection; chronic kidney disease; glomerular filtration rate; immune activation; inflammatory markers.
© The Author 2015. Published by Oxford University Press on behalf of the Infectious Diseases Society of America. All rights reserved. For Permissions, please e-mail: journals.permissions@oup.com.
Figures
References
-
- Breen EC, Rezai AR, Nakajima K, et al. Infection with HIV is associated with elevated IL-6 levels and production. J Immunol 1990; 144:480–4. - PubMed
-
- Wright SC, Jewett A, Mitsuyasu R, Bonavida B. Spontaneous cytotoxicity and tumor necrosis factor production by peripheral blood monocytes from AIDS patients. J Immunol 1988; 141:99–104. - PubMed
-
- Gage JR, Breen EC, Echeverri A, et al. Human herpesvirus 8-encoded interleukin 6 activates HIV-1 in the U1 monocytic cell line. AIDS 1999; 13:1851–5. - PubMed
-
- Ito M, Baba M, Sato A, et al. Tumor necrosis factor enhances replication of human immunodeficiency virus (HIV) in vitro. Biochem Biophys Res Commun 1989; 158:307–12. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- U01 AI035042/AI/NIAID NIH HHS/United States
- UL1 TR001079/TR/NCATS NIH HHS/United States
- U01-AI35040/AI/NIAID NIH HHS/United States
- U01-AI35042/AI/NIAID NIH HHS/United States
- U01 AI035041/AI/NIAID NIH HHS/United States
- UM1 AI035043/AI/NIAID NIH HHS/United States
- U01-AI35041/AI/NIAID NIH HHS/United States
- U01-AI35039/AI/NIAID NIH HHS/United States
- U01 AI035040/AI/NIAID NIH HHS/United States
- UL1-TR001079/TR/NCATS NIH HHS/United States
- U01 AI035039/AI/NIAID NIH HHS/United States
- UM1-AI35043/AI/NIAID NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
