

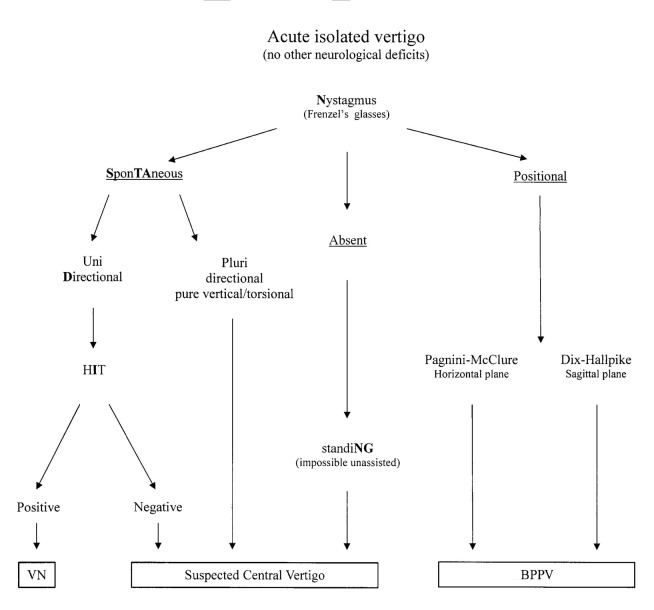
STANDING, a four-step bedside algorithm for differential diagnosis of acute vertigo in the Emergency Department
- PMID: 25762835
- PMCID: PMC4346998
STANDING, a four-step bedside algorithm for differential diagnosis of acute vertigo in the Emergency Department
Abstract
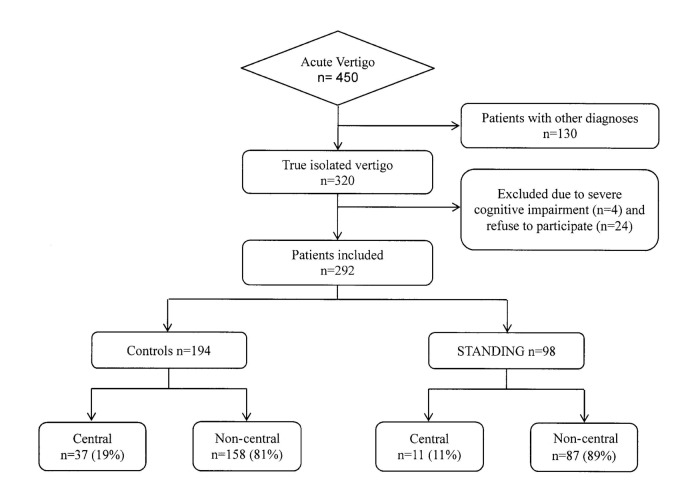
Vertigo is generally due to a benign disorder, but it is the most common symptom associated with misdiagnosis of stroke. In this pilot study, we preliminarily assessed the diagnostic performance of a structured bedside algorithm to differentiate central from non-central acute vertigo (AV). Adult patients presenting to a single Emergency Department with vertigo were evaluated with STANDING (SponTAneous Nystagmus, Direction, head Impulse test, standiNG) by one of five trained emergency physicians or evaluated ordinarily by the rest of the medical staff (control group). The gold standard was a complete audiologic evaluation by a clinicians who are experts in assessing dizzy patients and neuroimaging. Reliability, sensibility and specificity of STANDING were calculated. Moreover, to evaluate the potential clinical impact of STANDING, neuroimaging and hospitalisation rates were compared with control group. A total of 292 patients were included, and 48 (16.4%) had a diagnosis of central AV. Ninety-eight (33.4%) patients were evaluated with STANDING. The test had good interobserver agreement (k = 0.76), with very high sensitivity (100%, 95%CI 72.3-100%) and specificity (94.3%, 95%CI 90.7-94.3%). Furthermore, hospitalisation and neuroimaging test rates were lower in the STANDING than in the control group (27.6% vs. 50.5% and 31.6% vs. 71.1%, respectively). In conclusion, STANDING seems to be a promising simple structured bedside algorithm that in this preliminary study identified central AV with a very high sensitivity, and was associated with significant reduction of neuroimaging and hospitalisation rates.
La vertigine è generalmente dovuta ad una patologia benigna, ma rappresenta il sintomo più comunemente associato ad una mancata diagnosi di stroke. In questo studio pilota, abbiamo valutato in modo preliminare la validità diagnostica di un algoritmo bedside strutturato per differenziare le vertigini acute (VA) di origine centrale da quelle di origine non centrale. I pazienti adulti che si presentavano presso il nostro Dipartimento di Emergenza con vertigini venivano valutati con lo STANDING (SponTAneous Nystagmus Direction, head Impulse test, standiNG) da uno dei cinque medici del Pronto Soccorso adeguatamente istruiti, o in maniera tradizionale dal resto dello staff medico (gruppo di controllo). Il gold standard era rappresentato da una valutazione audiologica completa effettuata da un audiologo esperto e associata agli esami per immagini. Sono state calcolate la ripetibilità, la sensibilità e la specificità dello STANDING. Inoltre, per valutare in modo preliminare il potenziale impatto clinico dello STANDING, sono state confrontate le percentuali di richiesta di esami per immagini e di ospedalizzazioni con quelle del gruppo di controllo. Sono stati reclutati 292 pazienti, per 48 dei quali (16,4%) era stata diagnosticata una vertigine di origine centrale. Novantotto pazienti (33,4%) sono stati valutati con lo STANDING. L'intero algoritmo ha mostrato una buona concordanza tra gli esaminatori (K = 0,76), con una sensibilità (100%, 95%IC 72,3-100%) e una specificità (94,3%, 95%IC 90,7- 94,3%) molto alte. Inoltre, le percentuali di ospedalizzazione e di richiesta di esami per immagini sono state più basse nel gruppo valutato con lo STANDING rispetto al gruppo di controllo (rispettivamente 27,6% vs. 50,5% e 31,6% vs. 71,1%). In conclusione, lo STANDING sembra un algoritmo semplice e promettente, identificando nella nostra popolazione non selezionata le VA di origine centrale con un'alta sensibilità e con una riduzione significativa del numero di esami per immagini e ospedalizzazioni.
Keywords: Bedside algorithm; Benign paroxysmal positional vertigo; STANDING; Vestibular neuronitis.
Figures
References
-
- Newman-Toker DE, Cannon LM, Stofferahn ME, et al. Imprecision in patient reports of dizziness symptom quality: a cross-sectional study conducted in an acute care setting. Mayo Clin Proc. 2007;82:1329–1340. - PubMed
-
- Herr RD, Zun L, Mathews JJ. A directed approach to the dizzy patient. Ann Emerg Med. 1989;18:664–672. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical