

Review
doi: 10.5339/gcsp.2014.44.
eCollection 2014.
Reprogramming for cardiac regeneration
Affiliations
- PMID: 25763379
- PMCID: PMC4352683
- DOI: 10.5339/gcsp.2014.44
Item in Clipboard
Review
Reprogramming for cardiac regeneration
Glob Cardiol Sci Pract.
.
Abstract
Treatment of cardiovascular diseases remains challenging considering the limited regeneration capacity of the heart muscle. Developments of reprogramming strategies to create in vitro and in vivo cardiomyocytes have been the focus point of a considerable amount of research in the past decades. The choice of cells to employ, the state-of-the-art methods for different reprogramming strategies, and their promises and future challenges before clinical entry, are all discussed here.
Figures
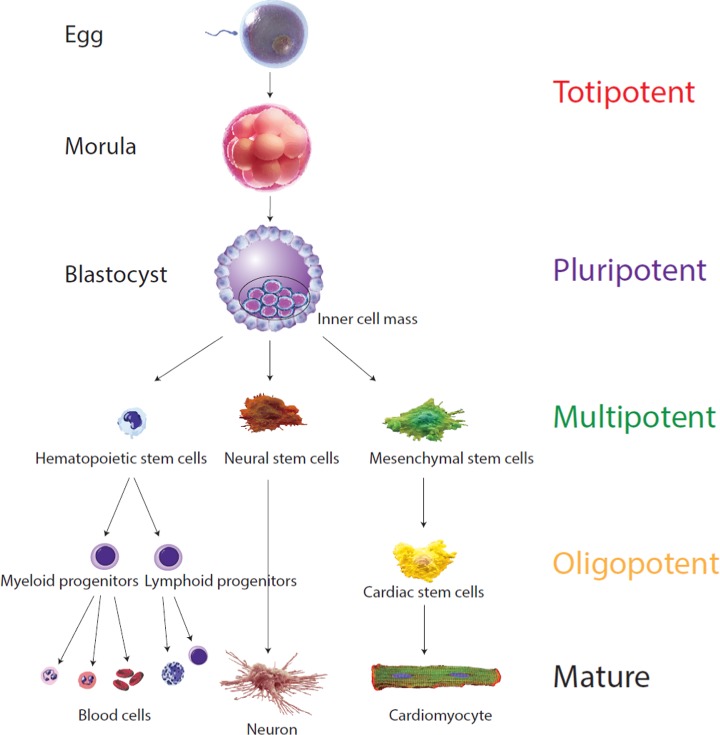
Different cells' “potency”. The “potency” of a cell is defined by the number of cell types it has the capacity to differentiate into. The fertilized egg is “totipotent”, cells having the potential to develop into an entire organism and therefore possesses the totality of potentials. This totipotent cell will divide in human for 4 days retaining this full capacity until a blastocyst develops, where these cells acquire some specialization. The cells from the inner cell mass cannot develop anymore into an entire organism, as they are unable to form the placenta but can still differentiate into all cell types within the organism. They are therefore qualified as “pluripotent”. Pluripotent cells will further multiply and acquire more specialization. The resulting “multipotent” cells retain the capacity to differentiate into various cell types. They are already specialized into ectoderm, endoderm or mesoderm. Finally, cells are considered “oligopotent” when they can only differentiate into very limited cell types (adapted from Ref.).
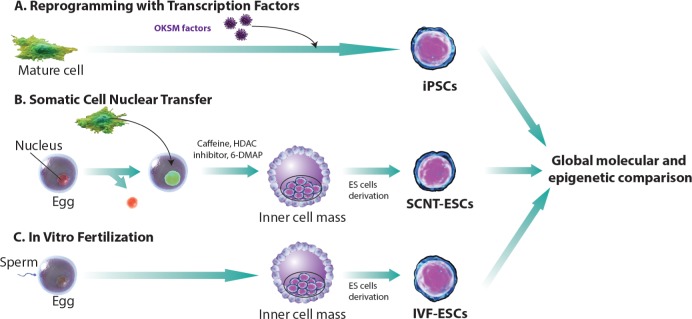
Comparing techniques for generating stem cells. There are three distinct ways to derive pluripotent stem cells in vitro. (A) iPS cell derivation is achieved via conversion of somatic cells with the addition of a cocktail of transcription factors, originally described as “Yamanaka factors”. (B) Tradtional embryonic stem cell derivation can be augmented by replacing the nucleus of an egg with a nucleus from a somatic cell at an early stage, as the cells mature and form the blastocyst. The inner cell mass (ICM) is isolated to form Nuclear Transfer embryonic stem (NT ES) cells. (C) In vitro fertilization is performed and ES cells are derived when reaching the blastocyte level to obtain IVF-ESCs (adapted from Ref.).
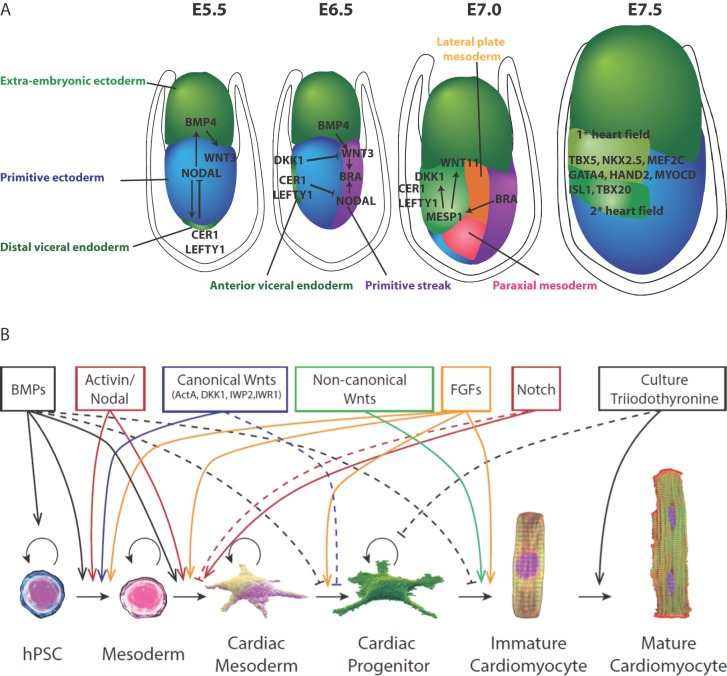
Lesson from embryology and factors involved in hPSC cardiac differentiation. (A) During mouse embryonic development at E5.5 gastrulation occurs by the formation of the primitive streak. An epithelial to mesenchymal transition (EMT) of anterior primitive ectoderm allows cells to move laterally between primitive ectoderm and visceral endoderm. At E6.5 cells located proximally to the primitive ectoderm go on to form the extraembryonic mesoderm. Cells adjacent to this zone form heart, blood and mesoderm derivatives. The most distal portion of the primitive streak gives rise to endoderm cells. At E7.0 the lateral plate mesoderm is formed which delaminates to form two layers. Cardiac mesoderm goes on to form the first heart field (FHF) laterally and more ventrally the second heart field (SHF) is formed both by coordinated expression of Dkk1, MESP1, Nodal and WNT signaling. Other cardiogenic signals, such as BMP and FGF, activate cardiac-specific transcription factors such as Nkx2.5, GATA4, HAND2, which coordinate to move both heart fields to the midline. Whereby at E7.5, the FHF progenitors form the heart tube which later contributes to the left ventricle. SHF progenitors join with the CMs of the FHF which leads to the rightward looping of the cardiac tube which eventually progresses towards formation of cardiac chambers. (B) Schematic representation of a family of factors reported to trigger progression from pluripotent state to CM (adapted from Ref.).
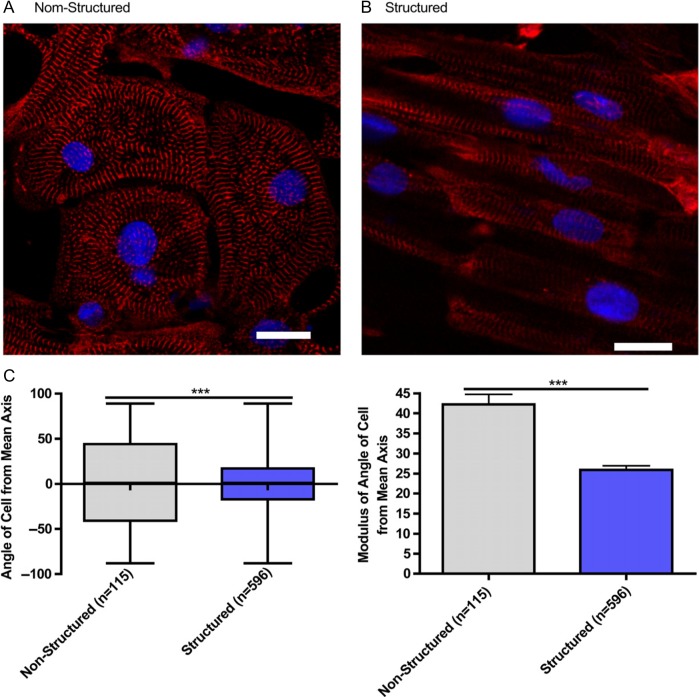
Microgrooved culture substrates' effect on calcium cycling of cardiac myocytes derived from human-induced pluripotent stem cells. Representative immunofluorescence of iPSC-CM cultured on unstructured polydimethylsiloxane (A) and microgrooved polydimethylsiloxane (B), Red - sarcomeric a-actin, Blue - DAPI, scale bar 20 mm.Quantification of cell alignment iPSC-CM on structured and unstructured constructs (C). (Adapted from Ref.)
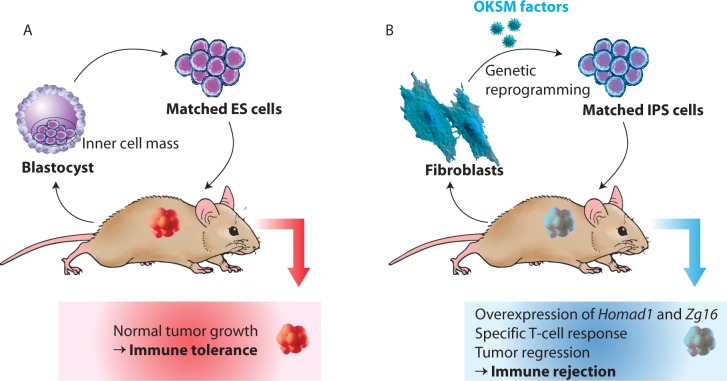
Immunogenicity of induced pluripotent stem cells. (A) Zhao et al. Performed transplantation studies assessed by injections of embryonic stem cells from the same genetic background found that ES cell-based transplants formed normal tumor growth. Hence, autologous ES cell transplantation evades immune system rejection. (B) Conversely, autologous iPS cells, derived from the same fetal fibroblasts, exhibited immunological rejection upon transplantation whilst in the same genetic background (adapted from Ref.).
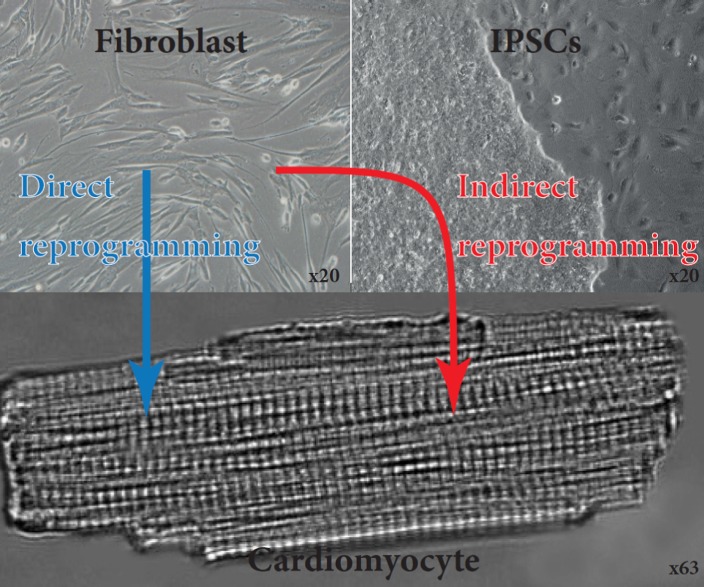
Generation of functional cardiomyocytes by direct and indirect reprogramming of fibroblasts. Fibroblasts derived from skin biopsy from a patient. These cells were then reprogrammed using OSKM factors towards induced pluripotent stem cells. These are then directed to differentiate towards CMs. Fibroblasts can also be directly reprogrammed towards CMs.
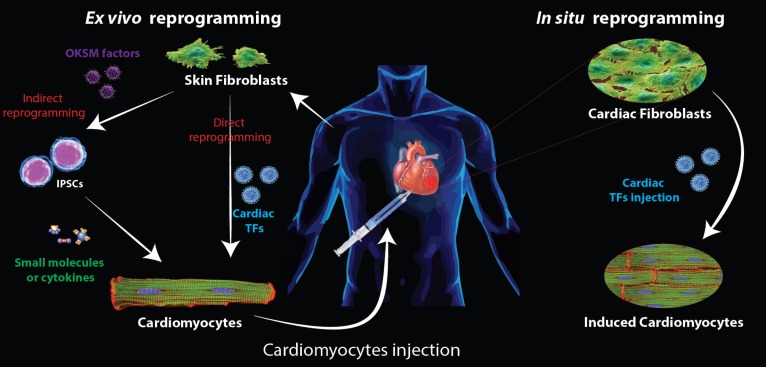
Schematic representation of heart repair strategies using reprogramming technologies Two strategies to repair post myocardial infarction are envisioned using in vitro reprogramming techniques starting from skin fibroblast. First fibroblasts are reprogrammed into iPSCs before being differentiated into CMs using small molecules or cytokines. The second approach consists of a direct reprogramming of the skin fibroblast into iCMs. In both cases, the CMs produced in vitro have to be injected into the patient. When considering in situ reprogramming, the transcription factors (carried by viruses) are directly delivered to the patient and TFs will be expressed in cardiac fibroblasts, reprogramming them directly into iCMs. OKSM factors: Oct4, Sox2, Klf4, c-Myc.
References
-
- Lancaster MA, Knoblich JA. Organogenesis in a dish: Modeling development and disease using organoid technologies. Science. 2014;345(6194):1247125. - PubMed
-
- Michael Fischberg JBG, Tom R. Elsdale nuclear transplantation in Xenopus laevis. Nature. 1958;(181):424.
-
- Takahashi K, Yamanaka S. Induction of pluripotent stem cells from mouse embryonic and adult fibroblast cultures by defined factors. Cell. 2006;126(4):663–676. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous