

Comparison of IVF Outcomes between Minimal Stimulation and High-Dose Stimulation for Patients with Poor Ovarian Reserve
- PMID: 25763403
- PMCID: PMC4334044
- DOI: 10.1155/2014/581451
Comparison of IVF Outcomes between Minimal Stimulation and High-Dose Stimulation for Patients with Poor Ovarian Reserve
Abstract
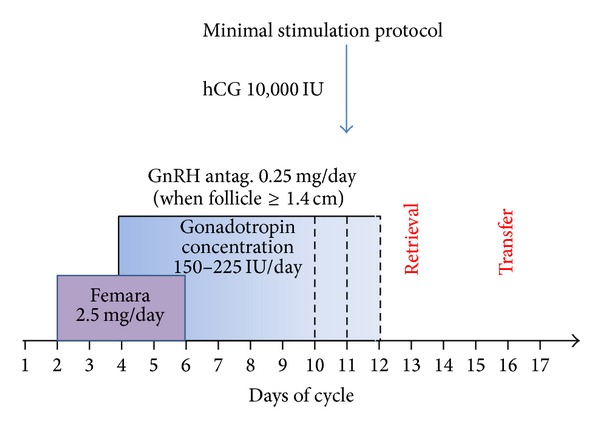
We examined whether treatment with minimum-dose stimulation (MS) protocol enhances clinical pregnancy rates compared to high-dose stimulation (HS) protocol. A retrospective cohort study was performed comparing IVF and pregnancy outcomes between MS and HS gonadotropin-antagonist protocol for patients with poor ovarian reserve (POR). Inclusion criteria included patients with an anti-Müllerian hormone (AMH) ≤8 pmol/L and/or antral follicle count (AFC) ≤5 on days 2-3 of the cycle. Patients from 2008 exclusively had a HS protocol treatment, while patients in 2010 had treatment with a MS protocol exclusively. The MS protocol involved letrozole at 2.5 mg over 5 days, starting from day 2, overlapping with gonadotropins, starting from the third day of letrozole at 150 units daily. GnRH antagonist was introduced once one or more follicles reached 14 mm or larger. The HS group received gonadotropins (≥300 IU/day) throughout their antagonist cycle. Clinical pregnancy rate was significantly higher in the MS protocol compared to the HS protocol (P = 0.007). Furthermore, the live birth rate was significantly higher in the MS group compare to the HS group (P = 0.034). In conclusion, the MS IVF protocol is less expensive (lower gonadotropin dosage) and resulted in a higher clinical pregnancy rate and live birth rate than a HS protocol for poor responders.
Figures
References
-
- Kyrou D, Kolibianakis EM, Venetis CA, Papanikolaou EG, Bontis J, Tarlatzis BC. How to improve the probability of pregnancy in poor responders undergoing in vitro fertilization: a systematic review and meta-analysis. Fertility and Sterility. 2009;91(3):749–766. - PubMed
-
- Klinkert ER, Broekmans FJM, Looman CWN, Habbema JDF, te Velde ER. Expected poor responders on the basis of an antral follicle count do not benefit from a higher starting dose of gonadotrophins in IVF treatment: a randomized controlled trial. Human Reproduction. 2005;20(3):611–615. - PubMed
-
- Zarek SM, Muasher SJ. Mild/minimal stimulation for in vitro fertilization: an old idea that needs to be revisited. Fertility & Sterility. 2011;95(8):2449–2455. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
