

One-year mortality rates in US children with end-stage renal disease
- PMID: 25766310
- PMCID: PMC4406829
- DOI: 10.1159/000380828
One-year mortality rates in US children with end-stage renal disease
Abstract
Background/aims: Few published data describe survival rates for pediatric end-stage renal disease (ESRD) patients. We aimed to describe one-year mortality rates for US pediatric ESRD patients over a 15-year period.
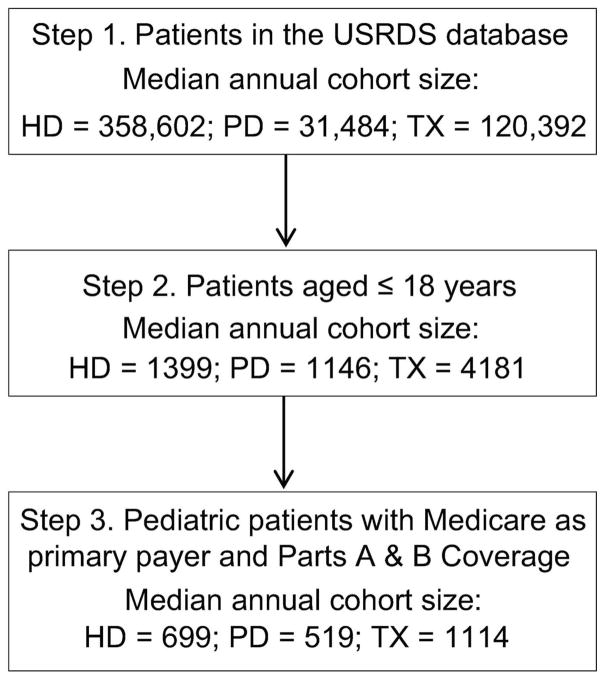
Methods: In this retrospective cohort study, we used the US Renal Data System database to identify period-prevalent cohorts of patients aged younger than 19 for each year during the period 1995-2010. Yearly cohorts averaged approximately 1,200 maintenance dialysis patients (60% hemodialysis, 40% peritoneal dialysis) and 1,100 transplant recipients. Patients were followed for up to 1 year and censored at change in modality, loss to follow-up, or death. We calculated the unadjusted model-based mortality rates per time at risk, within each cohort year, by treatment modality (hemodialysis, peritoneal dialysis, transplant) and patient characteristics; percentage of deaths by cause; and overall adjusted odds of mortality by characteristics and modality.
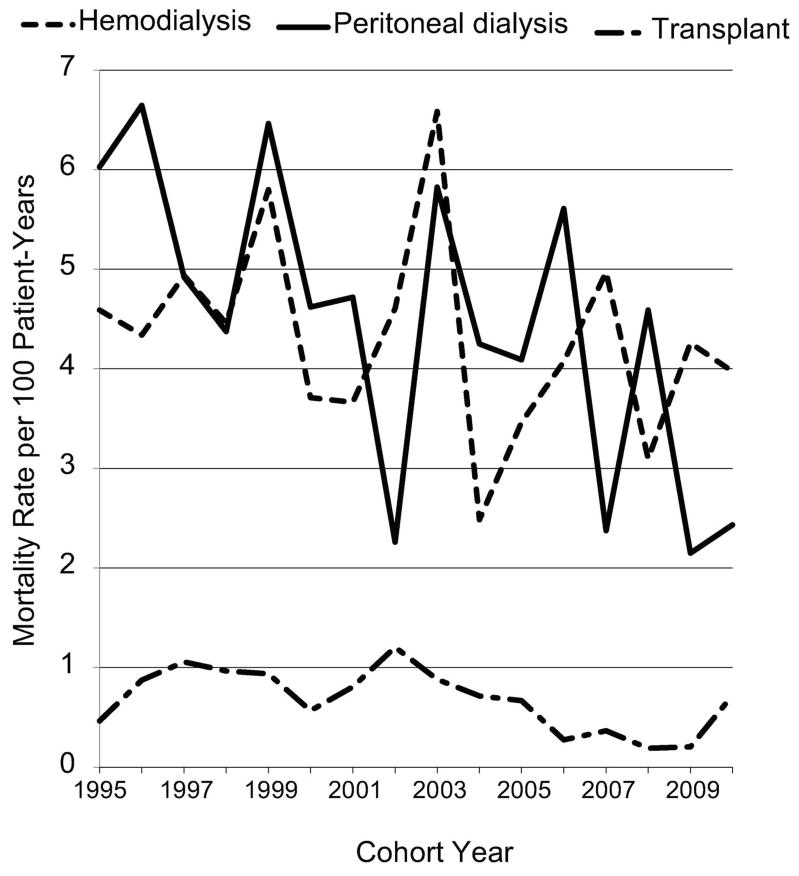
Results: Approximately 50% of patients were in the age group 15-18, 55% were male, and 45% were female. The most common causes of ESRD were congenital/reflux/obstructive causes (55%) and glomerulonephritis (30%). One-year mortality rates showed evidence of a decrease in the number of peritoneal dialysis patients (6.03 per 100 patient-years, 1995; 2.43, 2010; p = 0.0263). Mortality rates for transplant recipients (average 0.68 per 100 patient-years) were consistently lower than the rates for all dialysis patients (average 4.36 per 100 patient-years).
Conclusions: One-year mortality rates differ by treatment modality in pediatric ESRD patients.
Conflict of interest statement
The authors have no conflicts of interest with the study’s subject matter.
Figures
References
-
- U.S. Renal Data System. USRDS 2012 Annual Data Report: Atlas of Chronic Kidney Disease & End-Stage Renal Disease in the United States. 2012. Bethesda, MD: National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases; 2012.
-
- Ferris ME, Gipson DS, Kimmel PL, Eggers PW. Trends in treatment and outcomes of survival of adolescents initiating end-stage renal disease care in the United States of America. Pediatr Nephrol. 2006;21:1020–1026. - PubMed
-
- McDonald SP, Craig JC. Long-term survival of children with end-stage renal disease. N Engl J Med. 2004;350:2654–2662. - PubMed
-
- Collins AJ, Foley RN, Gilbertson DT, Chen SC. The state of chronic kidney disease, ESRD, and morbidity and mortality in the first year of dialysis. Clin J Am Soc Nephrol. 2009;4(Suppl 1):S5–S11. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
