

Comparison of the metabolic effects of ritonavir-boosted darunavir or atazanavir versus raltegravir, and the impact of ritonavir plasma exposure: ACTG 5257
- PMID: 25767256
- PMCID: PMC4660025
- DOI: 10.1093/cid/civ193
Comparison of the metabolic effects of ritonavir-boosted darunavir or atazanavir versus raltegravir, and the impact of ritonavir plasma exposure: ACTG 5257
Abstract
Background: Metabolic effects following combination antiretroviral therapy (cART) vary by regimen type. Changes in metabolic effects were assessed following cART in the AIDS Clinical Trials Group (ACTG) A5257 study, and correlated with plasma ritonavir trough concentrations (C24).
Methods: Treatment-naive adult subjects were randomized to ritonavir-boosted atazanavir or darunavir, or raltegravir-based cART. Changes in lipids and other metabolic outcomes over time were estimated. Differences between arms were estimated with 97.5% confidence intervals and compared using pairwise Student t tests. Associations between ritonavir C24 and lipid changes at week 48 were evaluated via linear regression.
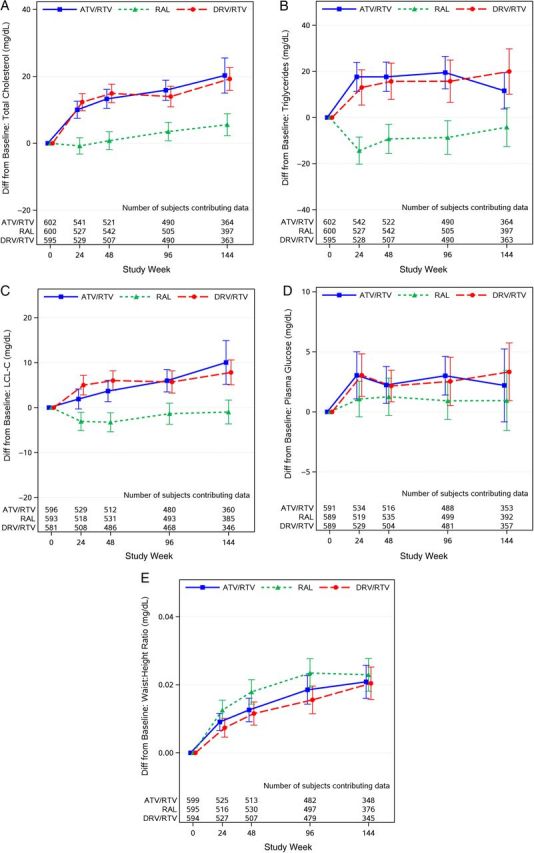
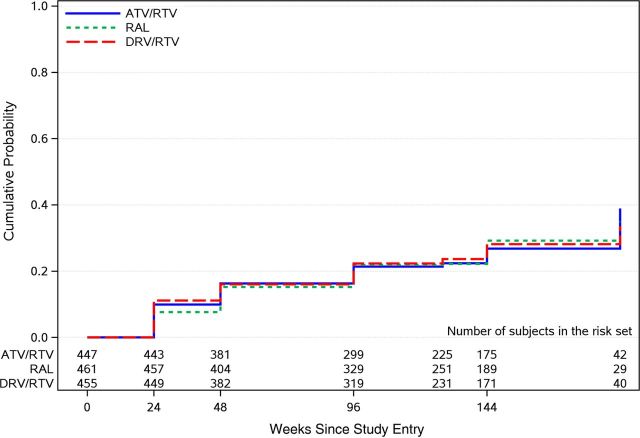
Results: Analyses included 1797 subjects with baseline fasting data. Baseline lipid profiles and metabolic syndrome rates (approximately 21%) were similar across arms. Comparable increases occurred in total cholesterol, triglycerides, and low-density lipoprotein cholesterol with the boosted protease inhibitors (PIs); each PI had greater increases relative to raltegravir (all P ≤ .001 at week 96). Metabolic syndrome incident rates by week 96 (approximately 22%) were not different across arms. Ritonavir C24 was not different by arm (P = .89) (median, 69 ng/mL and 74 ng/mL in the atazanavir and darunavir arms, respectively) and were not associated with changes in lipid measures (all P > .1).
Conclusions: Raltegravir produced the most favorable lipid profile. Metabolic syndrome rates were high at baseline and increased to the same degree in all arms. Ritonavir C24 was not different in the PI arms and had no relationship with the modest but comparable increases in lipids observed with either atazanavir or darunavir. The long-term clinical significance of the lipid changes noted with the PIs relative to raltegravir deserves further evaluation.
Clinical trials registration: NCT 00811954.
Trial registration: ClinicalTrials.gov NCT00811954.
Keywords: HIV/AIDS; cART; lipids; metabolic syndrome.
© The Author 2015. Published by Oxford University Press on behalf of the Infectious Diseases Society of America. All rights reserved. For Permissions, please e-mail: journals.permissions@oup.com.
Figures
References
-
- Panel on Antiretroviral Guidelines for Adults and Adolescents. Guidelines for the use of antiretroviral agents in HIV-1-infected adults and adolescents. Department of Health and Human Services, 2014:521–7. Available at: http://aidsinfo.nih.gov/ContentFiles/AdultandAdolescentGL.pdf Accessed 2 May 2014.
-
- World Health Organization. WHO consolidated guidelines on the use of antiretroviral drugs for treating and preventing HIV infection: recommendations for a public health approach. Geneva, Switzerland: WHO, 2013:1–272 Available at: http://www.who.int/hiv/pub/guidelines/arv2013/en/ Accessed 2 May 2014. - PubMed
-
- Periard D, Telenti A, Sudre P, et al. Atherogenic dyslipidemia in HIV-infected individuals treated with protease inhibitors. The Swiss HIV Cohort Study. Circulation 1999; 100:700–5. - PubMed
-
- Eron JJ, Young B, Cooper DA, et al. Switch to a raltegravir-based regimen versus continuation of a lopinavir-ritonavir-based regimen in stable HIV-infected patients with suppressed viraemia (SWITCHMRK 1 and 2): two multicentre, double-blind, randomised controlled trials. Lancet 2010; 375:396–407. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
- UM1AI68634/AI/NIAID NIH HHS/United States
- UL1 TR000058/TR/NCATS NIH HHS/United States
- UM1 AI069494/AI/NIAID NIH HHS/United States
- UM1 AI069423/AI/NIAID NIH HHS/United States
- U01 AI069412/AI/NIAID NIH HHS/United States
- UM1 AI069424/AI/NIAID NIH HHS/United States
- UM1 AI069471/AI/NIAID NIH HHS/United States
- UM1 AI069534/AI/NIAID NIH HHS/United States
- U01 AI069418/AI/NIAID NIH HHS/United States
- UM1 AI069415/AI/NIAID NIH HHS/United States
- P30 AI045008/AI/NIAID NIH HHS/United States
- UM1 AI069412/AI/NIAID NIH HHS/United States
- UM1 AI068634/AI/NIAID NIH HHS/United States
- P30 AI028697/AI/NIAID NIH HHS/United States
- UM1 AI069496/AI/NIAID NIH HHS/United States
- P30 AI027763/AI/NIAID NIH HHS/United States
- UM1 AI106701/AI/NIAID NIH HHS/United States
- UM1AI068636/AI/NIAID NIH HHS/United States
- UM1 AI068636/AI/NIAID NIH HHS/United States
- P30 AI050410/AI/NIAID NIH HHS/United States
- UM1 AI069418/AI/NIAID NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
