

The sympathetic nervous system alterations in human hypertension
- PMID: 25767284
- PMCID: PMC4367954
- DOI: 10.1161/CIRCRESAHA.116.303604
The sympathetic nervous system alterations in human hypertension
Abstract
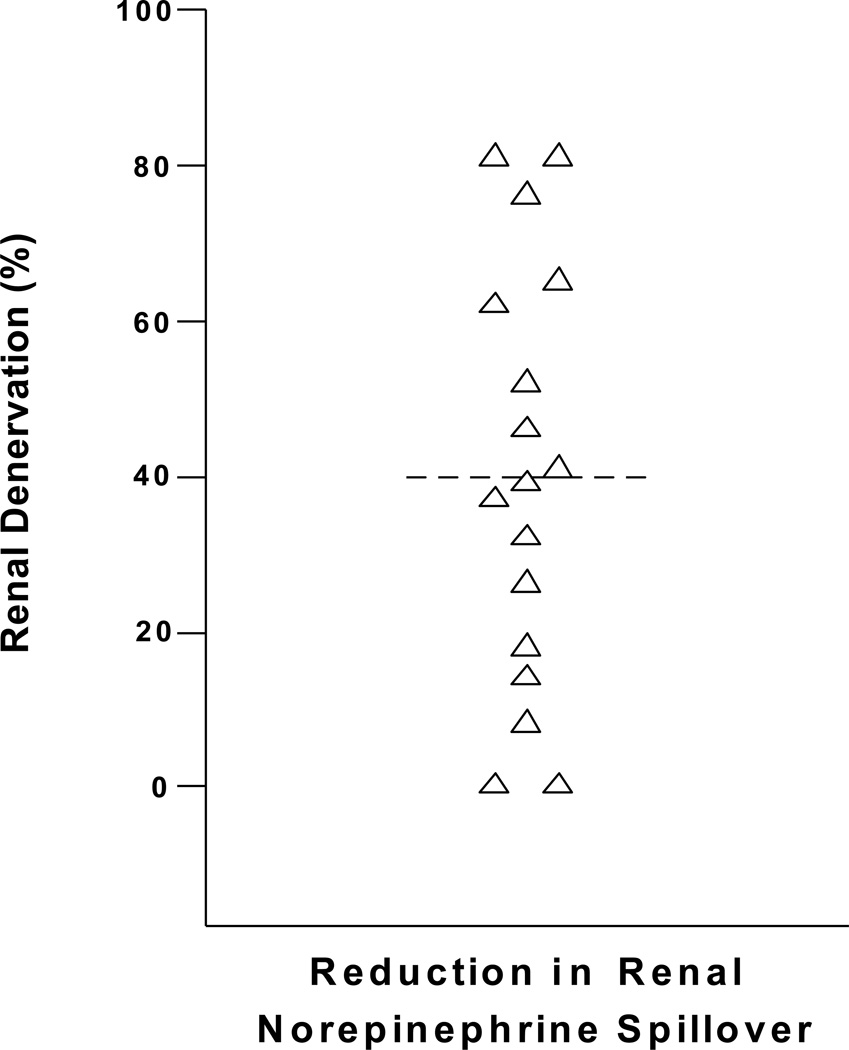
Several articles have dealt with the importance and mechanisms of the sympathetic nervous system alterations in experimental animal models of hypertension. This review addresses the role of the sympathetic nervous system in the pathophysiology and therapy of human hypertension. We first discuss the strengths and limitations of various techniques for assessing the sympathetic nervous system in humans, with a focus on heart rate, plasma norepinephrine, microneurographic recording of sympathetic nerve traffic, and measurements of radiolabeled norepinephrine spillover. We then examine the evidence supporting the importance of neuroadrenergic factors as promoters and amplifiers of human hypertension. We expand on the role of the sympathetic nervous system in 2 increasingly common forms of secondary hypertension, namely hypertension associated with obesity and with renal disease. With this background, we examine interventions of sympathetic deactivation as a mode of antihypertensive treatment. Particular emphasis is given to the background and results of recent therapeutic approaches based on carotid baroreceptor stimulation and radiofrequency ablation of the renal nerves.
Keywords: hypertension essential; renal insufficiency; sympathetic nervous system.
© 2015 American Heart Association, Inc.
Figures
Comment in
-
Renal Sympathetic Hyperactivity in Hypertension: True or False?Circ Res. 2016 Jul 22;119(3):e33-4. doi: 10.1161/CIRCRESAHA.116.309249. Circ Res. 2016. PMID: 27458198 No abstract available.
-
Response by Grassi et al to Letter Regarding Article, "The Sympathetic Nervous System Alterations in Human Hypertension".Circ Res. 2016 Jul 22;119(3):e35-6. doi: 10.1161/CIRCRESAHA.116.309261. Circ Res. 2016. PMID: 27458199 No abstract available.
References
-
- Shen MJ, Zipes DP. Role of the autonomic nervous system in modulating cardiac arrhythmias. Circ Res. 2014;114:1004–1021. - PubMed
-
- Leimbach WN, Jr, Wallin BG, Victor RG, Aylward PE, Sundlöf G, Mark AL. Direct evidence from intraneural recordings for increased central sympathetic outflow in patients with heart failure. Circulation. 1986;73:913–919. - PubMed
-
- Grassi G, Seravalle G, Cattaneo BM, Bolla GB, Lanfranchi A, Colombo M, Giannattasio C, Brunani A, Cavagnini F, Mancia G. Sympathetic activation in obese normotensive subjects. Hypertension. 1995;25:560–563. - PubMed
-
- Huggett RJ, Scott EM, Gilbey SG, Stoker JB, Mackintosh AF, Mary DA. Impact of type 2 diabetes mellitus on sympathetic neural mechanisms in hypertension. Circulation. 2003;108:3097–3101. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
