

Obesity-induced hypertension: interaction of neurohumoral and renal mechanisms
- PMID: 25767285
- PMCID: PMC4363087
- DOI: 10.1161/CIRCRESAHA.116.305697
Obesity-induced hypertension: interaction of neurohumoral and renal mechanisms
Abstract
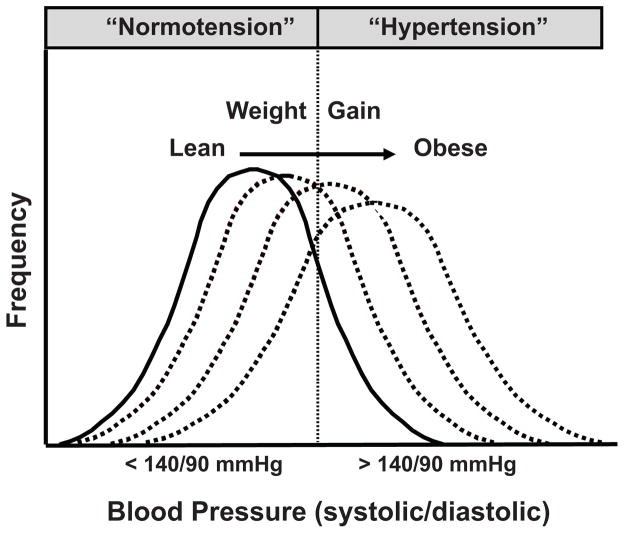
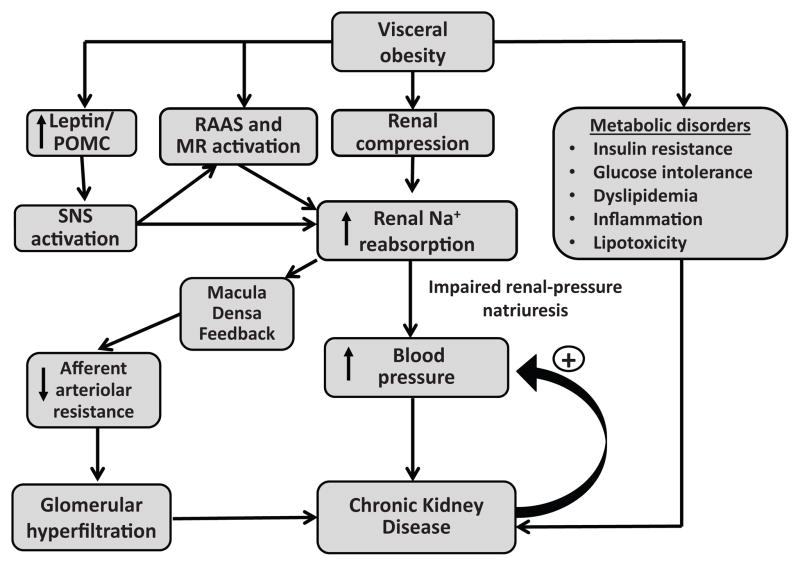
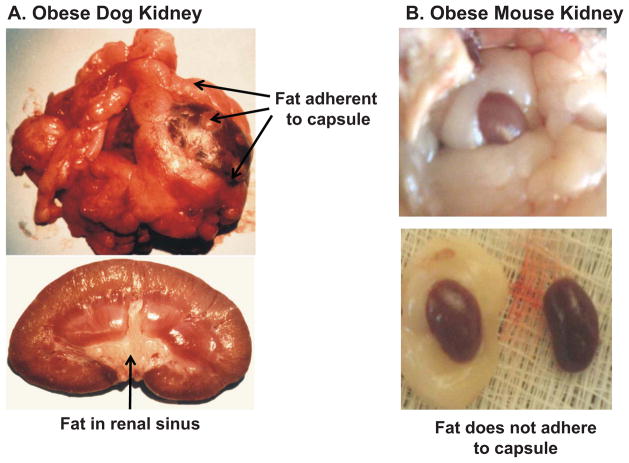
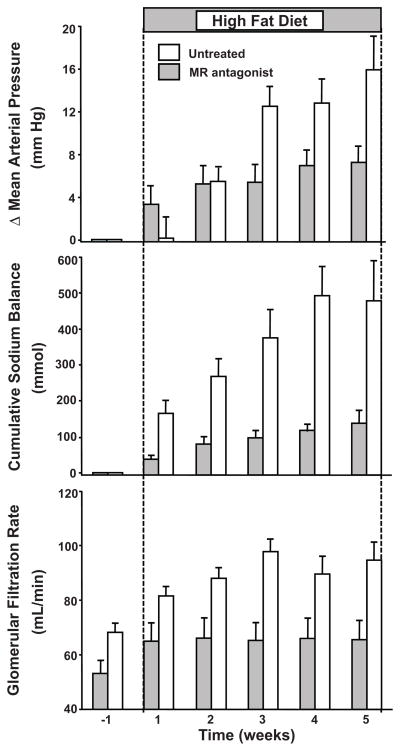
Excess weight gain, especially when associated with increased visceral adiposity, is a major cause of hypertension, accounting for 65% to 75% of the risk for human primary (essential) hypertension. Increased renal tubular sodium reabsorption impairs pressure natriuresis and plays an important role in initiating obesity hypertension. The mediators of abnormal kidney function and increased blood pressure during development of obesity hypertension include (1) physical compression of the kidneys by fat in and around the kidneys, (2) activation of the renin-angiotensin-aldosterone system, and (3) increased sympathetic nervous system activity. Activation of the renin-angiotensin-aldosterone system is likely due, in part, to renal compression, as well as sympathetic nervous system activation. However, obesity also causes mineralocorticoid receptor activation independent of aldosterone or angiotensin II. The mechanisms for sympathetic nervous system activation in obesity have not been fully elucidated but may require leptin and activation of the brain melanocortin system. With prolonged obesity and development of target organ injury, especially renal injury, obesity-associated hypertension becomes more difficult to control, often requiring multiple antihypertensive drugs and treatment of other risk factors, including dyslipidemia, insulin resistance and diabetes mellitus, and inflammation. Unless effective antiobesity drugs are developed, the effect of obesity on hypertension and related cardiovascular, renal and metabolic disorders is likely to become even more important in the future as the prevalence of obesity continues to increase.
Keywords: blood pressure; chronic renal insufficiency; kidney; leptin; melanocortins; mineralocorticoids.
© 2015 American Heart Association, Inc.
Figures
References
-
- Obesity and Overweight Fact Sheet N°311. 2014 http://www.who.int/mediacentre/factsheets/fs311/en/
-
- U.S.Department of Health and Human Services - Center for Disease Control and Prevention. 2014 http://www.cdc.gov/obesity/data/index.html.
-
- Hall JE. The kidney, hypertension, and obesity. Hypertension. 2003;41:625–633. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
