

Quality improvements in decreasing medication administration errors made by nursing staff in an academic medical center hospital: a trend analysis during the journey to Joint Commission International accreditation and in the post-accreditation era
- PMID: 25767393
- PMCID: PMC4354453
- DOI: 10.2147/TCRM.S79238
Quality improvements in decreasing medication administration errors made by nursing staff in an academic medical center hospital: a trend analysis during the journey to Joint Commission International accreditation and in the post-accreditation era
Abstract
Background: Medication errors may occur during prescribing, transcribing, prescription auditing, preparing, dispensing, administration, and monitoring. Medication administration errors (MAEs) are those that actually reach patients and remain a threat to patient safety. The Joint Commission International (JCI) advocates medication error prevention, but experience in reducing MAEs during the period of before and after JCI accreditation has not been reported.
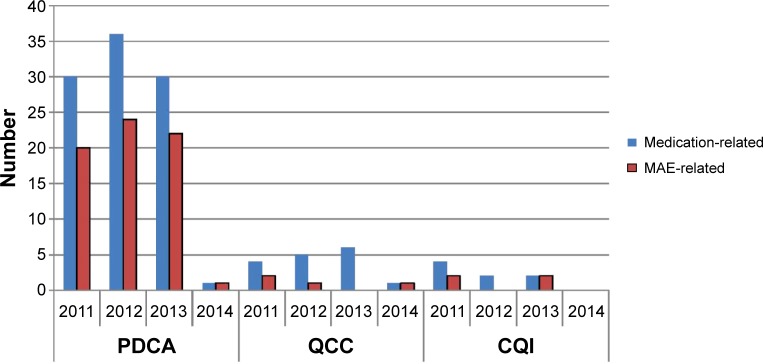
Methods: An intervention study, aimed at reducing MAEs in hospitalized patients, was performed in the Second Affiliated Hospital of Zhejiang University, Hangzhou, People's Republic of China, during the journey to JCI accreditation and in the post-JCI accreditation era (first half-year of 2011 to first half-year of 2014). Comprehensive interventions included organizational, information technology, educational, and process optimization-based measures. Data mining was performed on MAEs derived from a compulsory electronic reporting system.
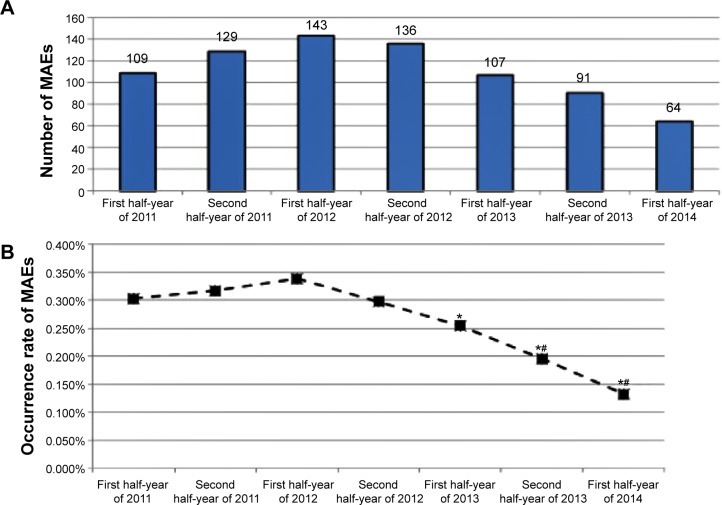
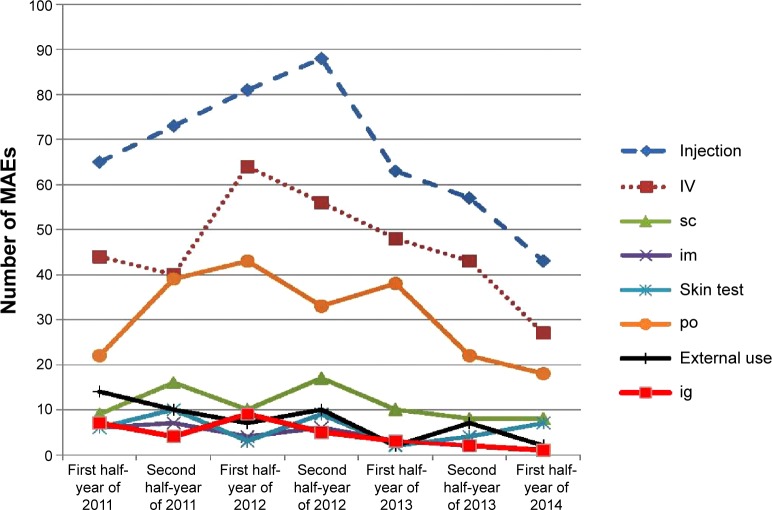
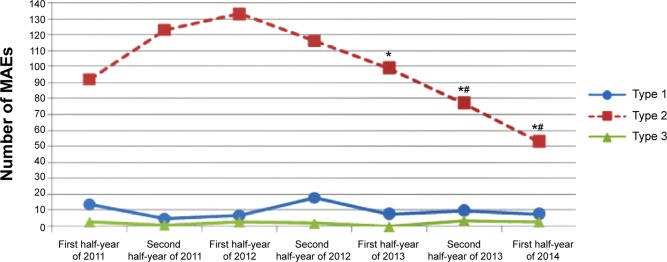
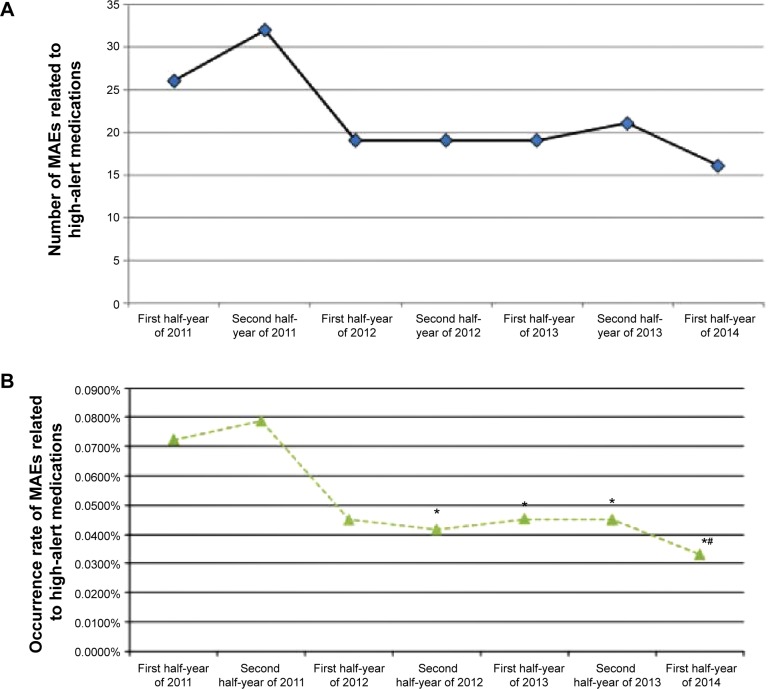
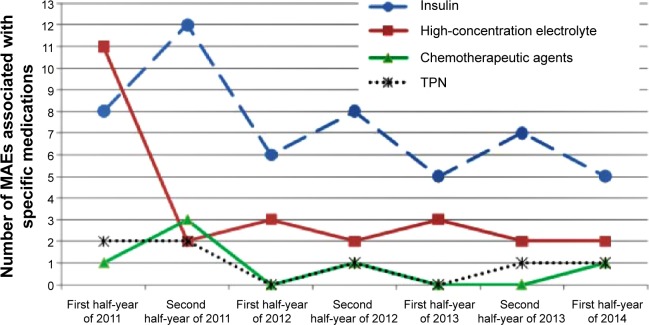
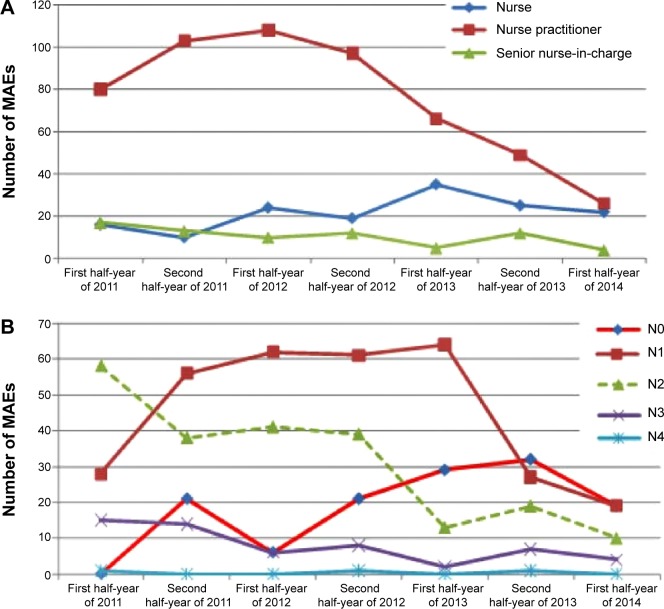
Results: The number of MAEs continuously decreased from 143 (first half-year of 2012) to 64 (first half-year of 2014), with a decrease in occurrence rate by 60.9% (0.338% versus 0.132%, P<0.05). The number of MAEs related to high-alert medications decreased from 32 (the second half-year of 2011) to 16 (the first half-year of 2014), with a decrease in occurrence rate by 57.9% (0.0787% versus 0.0331%, P<0.05). Omission was the top type of MAE during the first half-year of 2011 to the first half-year of 2014, with a decrease by 50% (40 cases versus 20 cases). Intravenous administration error was the top type of error regarding administration route, but it continuously decreased from 64 (first half-year of 2012) to 27 (first half-year of 2014). More experienced registered nurses made fewer medication errors. The number of MAEs in surgical wards was twice that in medicinal wards. Compared with non-intensive care units, the intensive care units exhibited higher occurrence rates of MAEs (1.81% versus 0.24%, P<0.001).
Conclusion: A 3-and-a-half-year intervention program on MAEs was confirmed to be effective. MAEs made by nursing staff can be reduced, but cannot be eliminated. The depth, breadth, and efficiency of multidiscipline collaboration among physicians, pharmacists, nurses, information engineers, and hospital administrators are pivotal to safety in medication administration. JCI accreditation may help health systems enhance the awareness and ability to prevent MAEs and achieve successful quality improvements.
Keywords: medication administration; medication errors; nurse; quality improvements.
Figures
References
-
- Haw C, Stubbs J, Dickens GL. Barriers to the reporting of medication administration errors and near misses: an interview study of nurses at a psychiatric hospital. J Psychiatr Ment Health Nurs. 2014;21(9):797–805. - PubMed
-
- Poon EG, Keohane CA, Yoon CS, et al. Effect of bar-code technology on the safety of medication administration. N Engl J Med. 2010;362(18):1698–1707. - PubMed
-
- Verrue CL, Mehuys E, Somers A, Van Maele G, Remon JP, Petrovic M. Medication administration in nursing homes: pharmacists’ contribution to error prevention. J Am Med Dir Assoc. 2010;11(4):275–283. - PubMed
-
- Kim J, Bates DW. Medication administration errors by nurses: adherence to guidelines. J Clin Nurs. 2013;22(3–4):590–598. - PubMed
LinkOut - more resources
Full Text Sources
