

Cost-effectiveness of clostridial collagenase ointment on wound closure in patients with diabetic foot ulcers: economic analysis of results from a multicenter, randomized, open-label trial
- PMID: 25767565
- PMCID: PMC4357050
- DOI: 10.1186/s13047-015-0065-x
Cost-effectiveness of clostridial collagenase ointment on wound closure in patients with diabetic foot ulcers: economic analysis of results from a multicenter, randomized, open-label trial
Erratum in
-
Erratum to: Cost-effectiveness of clostridial collagenase ointment on wound closure in patients with diabetic foot ulcers: economic analysis of results from a multicenter, randomized, open-label trial.J Foot Ankle Res. 2016 Aug 4;9:28. doi: 10.1186/s13047-016-0160-7. eCollection 2016. J Foot Ankle Res. 2016. PMID: 27493688 Free PMC article.
Abstract
Background: Approximately 10%-15% of people with diabetes develop at least one foot ulcer during their lifetime. Treatment of diabetic foot ulcers (DFUs) represents a significant economic burden. Enzymatic debridement with clostridial collagenase ointment (CCO) can be used to remove necrotic tissue from wounds. This study examined the impact of CCO as an effective adjunct therapy to serial sharp debridement (SSD) and assessed the cost-effectiveness of CCO compared with standard DFU treatments over 1 year.
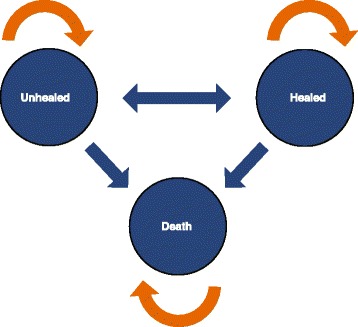
Methods: Adults 18 years or older with a diagnosis of type 1 or type 2 diabetes who had a neuropathic DFU were enrolled in a 12-week, randomized, open-label trial. Patients were randomly assigned to either treatment with CCO + SSD or to investigator-selected supportive care + SSD (Control). A 3-state Markov model with a 1-week cycle length was developed using wound-closure rates from the trial to estimate the number of healed-wound weeks and the expected DFU cost per patient. The 3 states included unhealed, healed, and death. Results were extrapolated to 1 year to estimate the number of healed-wound weeks per treatment and the average cost to achieve epithelialization. The perspective of the analysis was that of the payer, specifically, the third party payer.
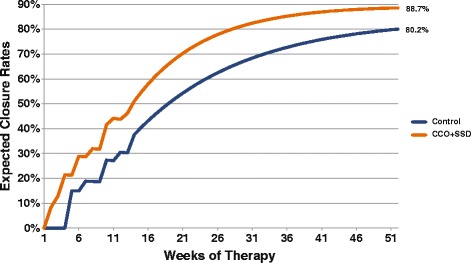
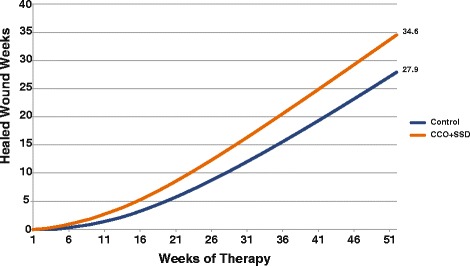
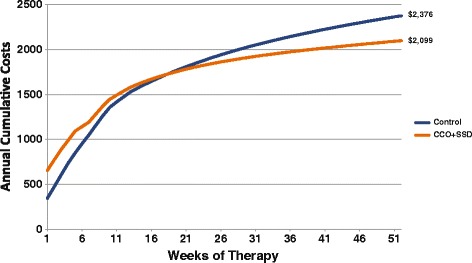
Results: The study sample included 55 patients (28 in CCO group; 27 Control). The majority were men (74.5%) with a mean age of 57.9 years. Projected healing rates were greater for the CCO + SSD group compared to Control (89% vs. 80%, respectively). The expected number of epithelialized weeks accumulated over 1 year was 25% greater in the CCO + SSD group than for Control (35 vs. 28 weeks, respectively). Over a 1-year time horizon, the expected cost per DFU was greater in the Control group than the CCO group ($2,376 vs. $2,099, respectively). The estimated cost per ulcer-free week was 40% higher for Control ($85/closed-wound week) than for CCO + SSD ($61/closed-wound week).
Conclusions: CCO + SSD therapy is a cost-effective method of debridement in the management of patients with DFUs, providing better outcomes at a lower cost. Further high quality trials are needed to confirm this finding.
Trial registration: This study was registered at ClinicalTrials.gov as NCT01408277.
Keywords: Clinical outcome; Collagenase; Cost-effectiveness; Debridement; Diabetes; Economic outcome; Foot ulcer; Health resource utilization; Wound healing.
Figures

References
-
- Lipsky BA. Infectious problems of the foot in diabetic patients. In: Bowker JH, Pfeifer MA, editors. Levin and O’Neal’s The Diabetic Foot. St. Louis: Mosby; 2001. pp. 467–80.
-
- Lavery LA, Armstrong DG, Wunderlich RP, Tredwell J, Boulton AJ. Diabetic foot syndrome: evaluating the prevalence and incidence of foot pathology in Mexican Americans and non-Hispanic whites from a diabetes disease management cohort. Diabetes Care. 2003;26:1435–8. doi: 10.2337/diacare.26.5.1435. - DOI - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
