

Role of endoscopy in multi-modality monitoring during aneurysm surgery: A single center experience with 175 consecutive unruptured aneurysms
- PMID: 25767585
- PMCID: PMC4352638
- DOI: 10.4103/1793-5482.151518
Role of endoscopy in multi-modality monitoring during aneurysm surgery: A single center experience with 175 consecutive unruptured aneurysms
Abstract
Objective and background: Unruptured aneurysm surgery is a challenge to all vascular neurosurgeons as the patient is asymptomatic and no even slight neurological deficits should be expected postoperatively. To this aim, multi-modality checking of the vessels during the surgery is highly recommended to assure of the patency of the parent and perforator arteries next to an aneurysm. In this paper, we present our experience in the last 1.5 years with emphasis on the role of endoscope assisted microsurgery.
Methods: One hundred and seventy-five patients with unruptured intracranial aneurysms were operated in our institute in the last 1½ years. All patients underwent endoscope assisted microsurgery with pre- and post-clipping indocyanine green angiography. In selected cases, motor evoked potential monitoring was implemented.
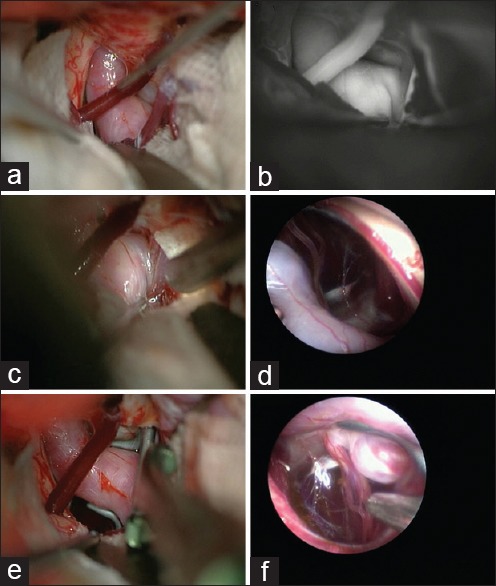
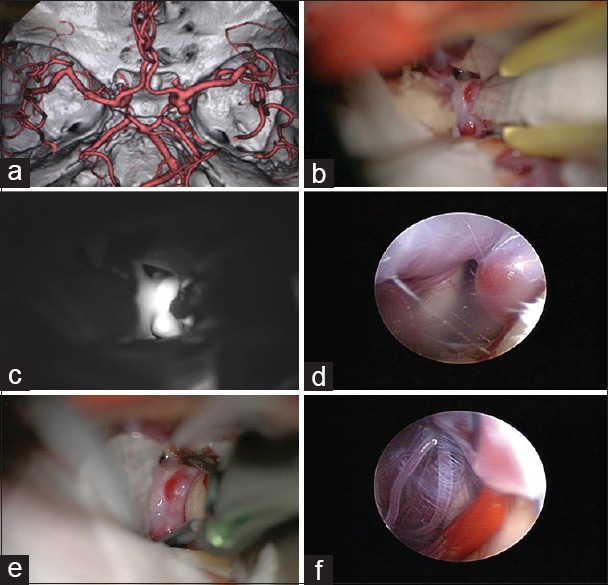
Results: No mortality was observed in this period, and only 6 patients (3.4%) suffered new permanent neurological deficits postoperatively. Our illustrative cases show how endoscopy may help the surgeon to visualize hidden vessels behind and medial to an aneurysm.
Conclusions: Our results indicated that multi-modality monitoring during unruptured aneurysm surgeries is associated with excellent outcome. Endoscope is able to show blind corners during aneurysm surgery which cannot be routinely observed with microscope and its application in aneurysm surgery assists the surgeon to make certain of complete neck clipping and preservation of perforating arteries around the aneurysm.
Keywords: Brain; clipping; endoscopy; monitoring; unruptured aneurysm.
Conflict of interest statement
Figures
References
-
- Lin N, Cahill KS, Frerichs KU, Friedlander RM, Claus EB. Treatment of ruptured and unruptured cerebral aneurysms in the USA: A paradigm shift. J Neurointerv Surg. 2012;4:182–9. - PubMed
-
- Aydin Y, Cavusoglu H, Kahyaoglu O, Müslüman AM, Yilmaz A, Türkmenoglu ON, et al. Clip ligation of unruptured intracranial aneurysms: A prospective midterm outcome study. Acta Neurochir (Wien) 2012;154:1135–44. - PubMed
-
- Motoyama Y, Kawaguchi M, Yamada S, Nakagawa I, Nishimura F, Hironaka Y, et al. Evaluation of combined use of transcranial and direct cortical motor evoked potential monitoring during unruptured aneurysm surgery. Neurol Med Chir (Tokyo) 2011;51:15–22. - PubMed
-
- Oda J, Kato Y, Chen SF, Sodhiya P, Watabe T, Imizu S, et al. Intraoperative near-infrared indocyanine green-videoangiography (ICG-VA) and graphic analysis of fluorescence intensity in cerebral aneurysm surgery. J Clin Neurosci. 2011;18:1097–100. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources