

Vascular calcification in patients with nondialysis CKD over 3 years
- PMID: 25770175
- PMCID: PMC4386255
- DOI: 10.2215/CJN.07450714
Vascular calcification in patients with nondialysis CKD over 3 years
Abstract
Background and objectives: Vascular calcification (VC) is common in CKD, but little is known about its prognostic effect on patients with nondialysis CKD. The prevalence of VC and its ability to predict death, time to hospitalization, and renal progression were assessed.
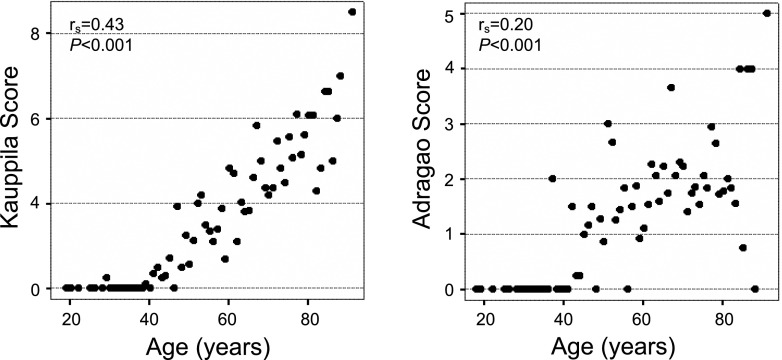
Design, setting, participants, & measurements: The Study of Mineral and Bone Disorders in CKD in Spain is a prospective, observational, 3-year follow-up study of 742 patients with nondialysis CKD stages 3-5 from 39 centers in Spain from April to May 2009. VC was assessed using Adragao (AS; x-ray pelvis and hands) and Kauppila (KS; x-ray lateral lumbar spine) scores from 572 and 568 patients, respectively. The primary end point was death. Secondary outcomes were hospital admissions and appearance of a combined renal end point (beginning of dialysis or drop >30% in eGFR). Factors related to VC were assessed by logistic regression analysis. Survival analysis was assessed by Cox proportional models.
Results: VC was present in 79% of patients and prominent in 47% (AS≥3 or KS>6). Age (odds ratio [OR], 1.05; 95% confidence interval [95% CI], 1.02 to 1.07; P<0.001), phosphorous (OR, 1.68; 95% CI, 1.28 to 2.20; P<0.001), and diabetes (OR, 2.11; 95% CI, 1.32 to 3.35; P=0.002) were independently related to AS≥3. After a median follow-up of 35 months (interquartile range=17-36), there were 70 deaths (10%). After multivariate adjustment for age, smoking, diabetes, comorbidity, renal function, and level of phosphorous, AS≥3 but not KS>6 was independently associated with all-cause (hazard ratio [HR], 2.07; 95% CI, 1.07 to 4.01; P=0.03) and cardiovascular (HR, 3.46; 95% CI, 1.27 to 9.45; P=0.02) mortality as well as a shorter hospitalization event-free period (HR, 1.14; 95% CI, 1.06 to 1.22; P<0.001). VC did not predict renal progression.
Conclusions: VC is highly prevalent in patients with CKD. VC assessment using AS independently predicts death and time to hospitalization. Therefore, it could be a useful index to identify patients with CKD at high risk of death and morbidity as previously reported in patients on dialysis.
Keywords: cardiovascular disease; chronic renal disease; metabolism; mineral; vascular calcification.
Copyright © 2015 by the American Society of Nephrology.
Figures



Comment in
-
Vascular calcification in predialysis CKD: common and deadly.Clin J Am Soc Nephrol. 2015 Apr 7;10(4):551-3. doi: 10.2215/CJN.01940215. Epub 2015 Mar 13. Clin J Am Soc Nephrol. 2015. PMID: 25770177 Free PMC article. No abstract available.
References
-
- Russo D, Palmiero G, De Blasio AP, Balletta MM, Andreucci VE: Coronary artery calcification in patients with CRF not undergoing dialysis. Am J Kidney Dis 44: 1024–1030, 2004 - PubMed
-
- Garland JS, Holden RM, Groome PA, Lam M, Nolan RL, Morton AR, Pickett W: Prevalence and associations of coronary artery calcification in patients with stages 3 to 5 CKD without cardiovascular disease. Am J Kidney Dis 52: 849–858, 2008 - PubMed
-
- García-Canton C, Bosch E, Ramírez A, Gonzalez Y, Auyanet I, Guerra R, Perez MA, Fernández E, Toledo A, Lago M, Checa MD: Vascular calcification and 25-hydroxyvitamin D levels in non-dialysis patients with chronic kidney disease stages 4 and 5. Nephrol Dial Transplant 26: 2250–2256, 2011 - PubMed
-
- Toussaint ND, Lau KK, Strauss BJ, Polkinghorne KR, Kerr PG: Associations between vascular calcification, arterial stiffness and bone mineral density in chronic kidney disease. Nephrol Dial Transplant 23: 586–593, 2008 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
