

Understanding the causes of intravenous medication administration errors in hospitals: a qualitative critical incident study
- PMID: 25770226
- PMCID: PMC4360808
- DOI: 10.1136/bmjopen-2014-005948
Understanding the causes of intravenous medication administration errors in hospitals: a qualitative critical incident study
Abstract
Objectives: To investigate the underlying causes of intravenous medication administration errors (MAEs) in National Health Service (NHS) hospitals.
Setting: Two NHS teaching hospitals in the North West of England.
Participants: Twenty nurses working in a range of inpatient clinical environments were identified and recruited using purposive sampling at each study site.
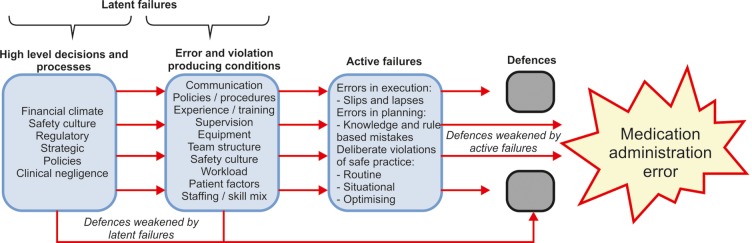
Primary outcome measures: Semistructured interviews were conducted with nurse participants using the critical incident technique, where they were asked to discuss perceived causes of intravenous MAEs that they had been directly involved with. Transcribed interviews were analysed using the Framework approach and emerging themes were categorised according to Reason's model of accident causation.
Results: In total, 21 intravenous MAEs were discussed containing 23 individual active failures which included slips and lapses (n=11), mistakes (n=8) and deliberate violations of policy (n=4). Each active failure was associated with a range of error and violation provoking conditions. The working environment was implicated when nurses lacked healthcare team support and/or were exposed to a perceived increased workload during ward rounds, shift changes or emergencies. Nurses frequently reported that the quality of intravenous dose-checking activities was compromised due to high perceived workload and working relationships. Nurses described using approaches such as subconscious functioning and prioritising to manage their duties, which at times contributed to errors.
Conclusions: Complex interactions between active and latent failures can lead to intravenous MAEs in hospitals. Future interventions may need to be multimodal in design in order to mitigate these risks and reduce the burden of intravenous MAEs.
Keywords: QUALITATIVE RESEARCH.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://group.bmj.com/group/rights-licensing/permissions.
Figures
References
-
- Kanjanarat P, Winterstein AG, Johns TE et al. . Nature of preventable adverse drug events in hospitals: a literature review. Am J Health Syst Pharm 2003;60:1750–9. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical