

Clinical decision rule for primary care patient with acute low back pain at risk of developing chronic pain
- PMID: 25771757
- PMCID: PMC4475413
- DOI: 10.1016/j.spinee.2015.03.003
Clinical decision rule for primary care patient with acute low back pain at risk of developing chronic pain
Abstract
Background context: Primary care clinicians need to identify candidates for early interventions to prevent patients with acute pain from developing chronic pain.
Purpose: We conducted a 2-year prospective cohort study of risk factors for the progression to chronic pain and developed and internally validated a clinical decision rule (CDR) that stratifies patients into low-, medium-, and high-risk groups for chronic pain.
Study design/setting: This is a prospective cohort study in primary care.
Patient sample: Patients with acute low back pain (LBP, ≤30 days duration) were included.
Outcome measures: Outcome measures were self-reported perceived nonrecovery and chronic pain.
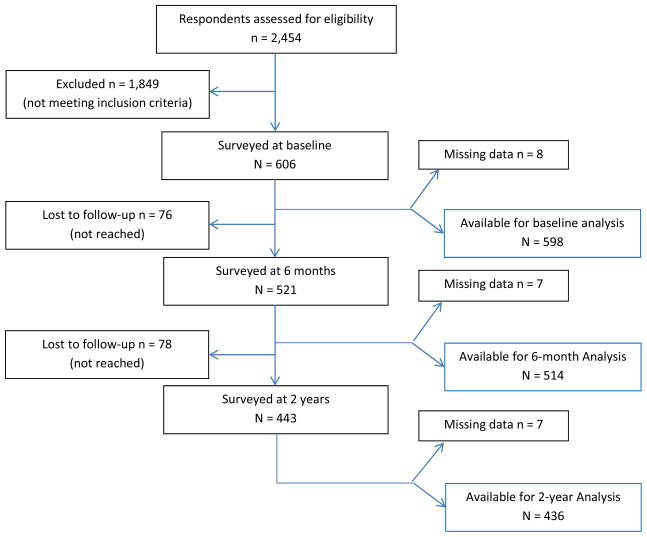
Methods: Patients were surveyed at baseline, 6 months, and 2 years. We conducted bivariate and multivariate regression analyses of demographic, clinical, and psychosocial variables for chronic pain outcomes, developed a CDR, and assessed its performance by calculating the bootstrapped areas under the receiver-operating characteristic curve (AUC) and likelihood ratios.
Results: Six hundred five patients enrolled: 13% had chronic pain at 6 months and 19% at 2 years. An eight-item CDR was most parsimonious for classifying patients into three risk levels. Bootstrapped AUC was 0.76 (0.70-0.82) for the 6-month CDR. Each 10-point score increase (60-point range) was associated with an odds ratio of 11.1 (10.8-11.4) for developing chronic pain. Using a less than 5% probability of chronic pain as the cutoff for low risk and a greater than 40% probability for high risk, likelihood ratios were 0.26 (0.14-0.48) and 4.4 (3.0-6.3) for these groups, respectively.
Conclusions: A CDR was developed that may help primary care clinicians classify patients with strictly defined acute LBP into low-, moderate-, and high-risk groups for developing chronic pain and performed acceptably in 1,000 bootstrapped replications. Validation in a separate sample is needed.
Keywords: Acute pain; Chronic pain; Clinical decision rule; Low back pain; Prediction; Primary care.
Copyright © 2015 Elsevier Inc. All rights reserved.
References
-
- Von Korff M, Saunders K. The course of back pain in primary care. Spine. 1996;21(24):2833–2837. discussion 2838–2839. - PubMed
-
- Dagenais S, Caro J, Haldeman S. A systematic review of low back pain cost of illness studies in the United States and internationally. Spine J. 2008;8(1):8–20. - PubMed
-
- Borkan J, Van Tulder M, Reis S, Schoene ML, Croft P, Hermoni D. Advances in the field of low back pain in primary care: a report from the fourth international forum. Spine. 2002;27(5):E128–132. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
