

Neuraxial blockade for external cephalic version: Cost analysis
- PMID: 25771920
- PMCID: PMC5637526
- DOI: 10.1111/jog.12674
Neuraxial blockade for external cephalic version: Cost analysis
Abstract
Aim: Neuraxial blockade (epidural or spinal anesthesia/analgesia) with external cephalic version increases the external cephalic version success rate. Hospitals and insurers may affect access to neuraxial blockade for external cephalic version, but the costs to these institutions remain largely unstudied. The objective of this study was to perform a cost analysis of neuraxial blockade use during external cephalic version from hospital and insurance payer perspectives. Secondarily, we estimated the effect of neuraxial blockade on cesarean delivery rates.
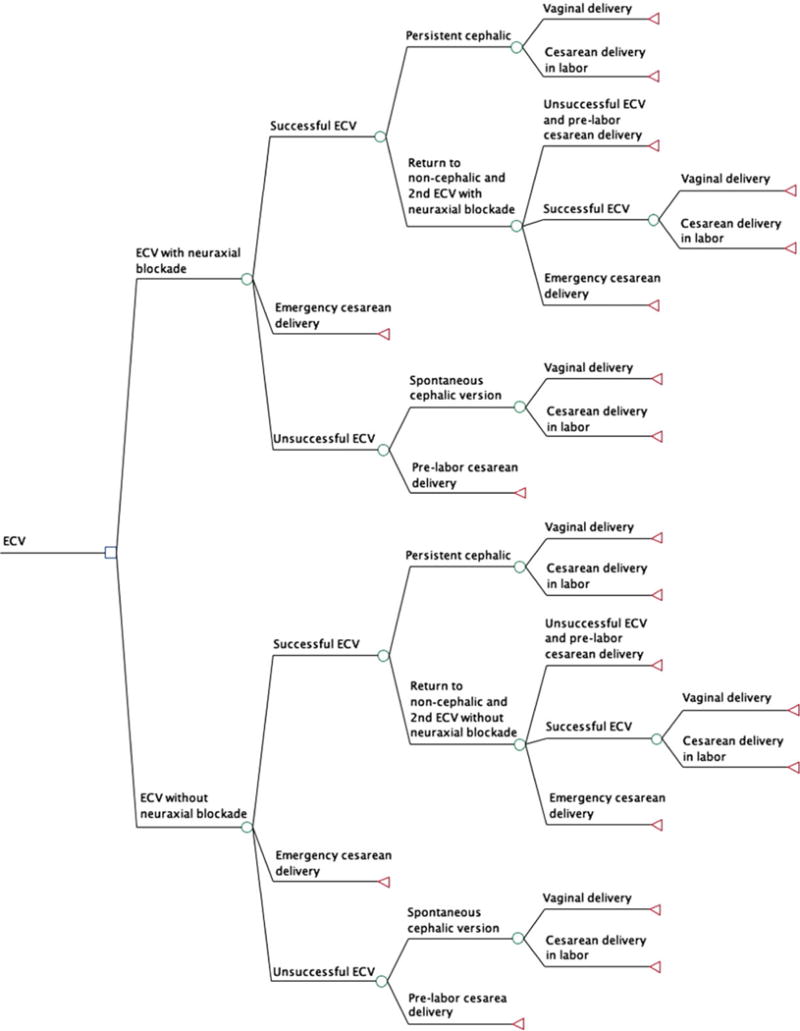
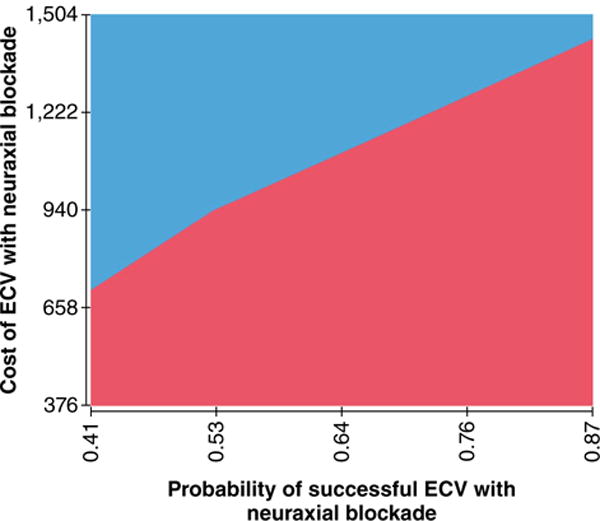
Methods: A decision-analysis model was developed using costs and probabilities occurring prenatally through the delivery hospital admission. Model inputs were derived from the literature, national databases, and local supply costs. Univariate and bivariate sensitivity analyses and Monte Carlo simulations were performed to assess model robustness.
Results: Neuraxial blockade was cost saving to both hospitals ($30 per delivery) and insurers ($539 per delivery) using baseline estimates. From both perspectives, however, the model was sensitive to multiple variables. Monte Carlo simulation indicated neuraxial blockade to be more costly in approximately 50% of scenarios. The model demonstrated that routine use of neuraxial blockade during external cephalic version, compared to no neuraxial blockade, prevented 17 cesarean deliveries for every 100 external cephalic versions attempted.
Conclusions: Neuraxial blockade is associated with minimal hospital and insurer cost changes in the setting of external cephalic version, while reducing the cesarean delivery rate.
Keywords: breech; cesarean delivery; cost; external cephalic version; neuraxial blockade.
© 2015 The Authors. Journal of Obstetrics and Gynaecology Research © 2015 Japan Society of Obstetrics and Gynecology.
Conflict of interest statement
The authors have no financial conflicts of interest to disclose.
Figures
Similar articles
-
Anesthetic management of external cephalic version.Clin Perinatol. 2013 Sep;40(3):399-412. doi: 10.1016/j.clp.2013.06.001. Epub 2013 Jul 23. Clin Perinatol. 2013. PMID: 23972747 Review.
-
Brief report: a cost analysis of neuraxial anesthesia to facilitate external cephalic version for breech fetal presentation.Anesth Analg. 2013 Jul;117(1):155-9. doi: 10.1213/ANE.0b013e31828e5bc7. Epub 2013 Apr 16. Anesth Analg. 2013. PMID: 23592608 Review.
-
Lessons learned from a single institution's retrospective analysis of emergent cesarean delivery following external cephalic version with and without neuraxial anesthesia.Int J Obstet Anesth. 2017 May;31:57-62. doi: 10.1016/j.ijoa.2017.03.012. Epub 2017 Apr 2. Int J Obstet Anesth. 2017. PMID: 28499551
-
Survey of external cephalic version for breech presentation and neuraxial blockade use.J Clin Anesth. 2016 Nov;34:616-22. doi: 10.1016/j.jclinane.2016.05.040. Epub 2016 Jul 28. J Clin Anesth. 2016. PMID: 27687460
-
Central neuraxial blockade promotes external cephalic version success after a failed attempt.Anesth Analg. 2002 Jun;94(6):1589-92, table of contents. doi: 10.1097/00000539-200206000-00041. Anesth Analg. 2002. PMID: 12032033
References
-
- Hannah ME, Hannah WJ, Hewson SA, Hodnett ED, Saigal S, Willan AR. Planned caesarean section versus planned vaginal birth for breech presentation at term: A randomised multicentre trial. Term Breech Trial Collaborative Group. Lancet. 2000;356:1375–1383. - PubMed
-
- Hehir M, O’Connor HD, Kent EM, et al. Changes in vaginal breech delivery rates in a single large metropolitan area. Am J Obstet Gynecol. 2012;206:498e1–498.e4. - PubMed
-
- American College of Obstetrician Gynecologists. ACOG practice bulletin #13. ECV Obstet Gynecol. 2000;13:380–385.
-
- Kok J, Cnossen J, Gravendeel L, van der Post J, Opmeer B, Mol B. Clinical factors to predict the outcome of external cephalic version: A metaanalysis. Am J Obstet Gynecol. 2008;199:630.e1–630.e7. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
