

Discrimination in Healthcare Settings is Associated with Disability in Older Adults: Health and Retirement Study, 2008-2012
- PMID: 25773918
- PMCID: PMC4579241
- DOI: 10.1007/s11606-015-3233-6
Discrimination in Healthcare Settings is Associated with Disability in Older Adults: Health and Retirement Study, 2008-2012
Abstract
Background: As our society ages, improving medical care for an older population will be crucial. Discrimination in healthcare may contribute to substandard experiences with the healthcare system, increasing the burden of poor health in older adults. Few studies have focused on the presence of healthcare discrimination and its effects on older adults.
Objective: We aimed to examine the relationship between healthcare discrimination and new or worsened disability.
Design: This was a longitudinal analysis of data from the nationally representative Health and Retirement Study administered in 2008 with follow-up through 2012.
Participants: Six thousand and seventeen adults over the age of 50 years (mean age 67 years, 56.3 % female, 83.1 % white) were included in this study.
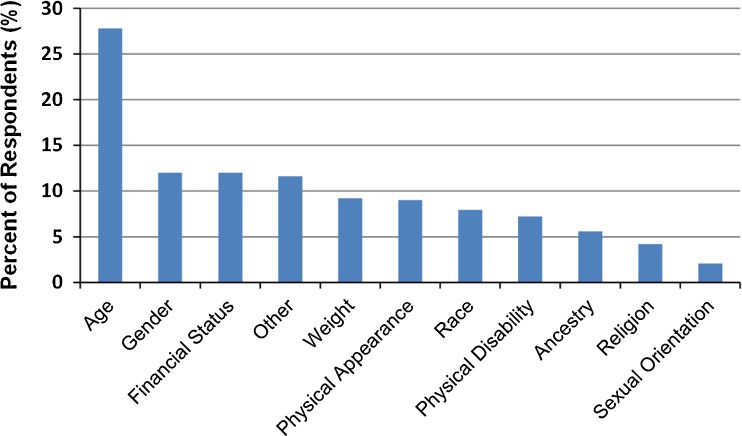
Main measures: Healthcare discrimination assessed by a 2008 report of receiving poorer service or treatment than other people by doctors or hospitals (never, less than a year=infrequent; more than once a year=frequent). Outcome was self-report of new or worsened disability by 2012 (difficulty or dependence in any of six activities of daily living). We used a Cox proportional hazards model adjusting for age, race/ethnicity, gender, net worth, education, depression, high blood pressure, diabetes, cancer, lung disease, heart disease, stroke, and healthcare utilization in the past 2 years.
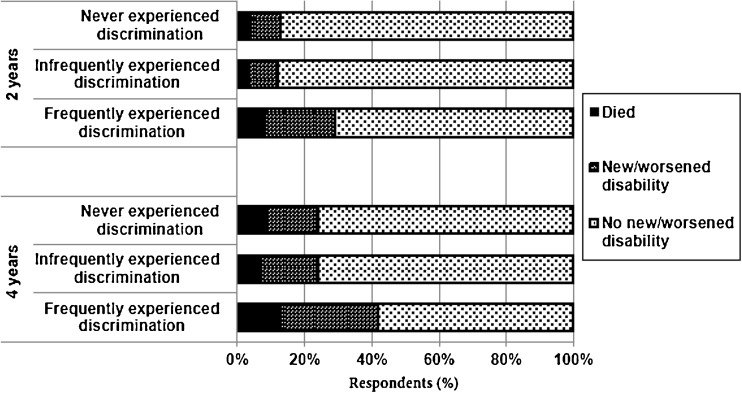
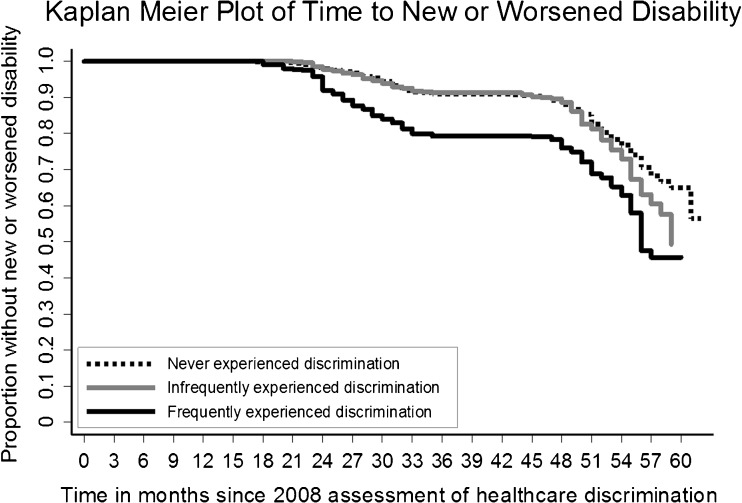
Key results: In all, 12.6 % experienced discrimination infrequently and 5.9 % frequently. Almost one-third of participants (29 %) reporting frequent healthcare discrimination developed new or worsened disability over 4 years, compared to 16.8 % of those who infrequently and 14.7 % of those who never experienced healthcare discrimination (p < 0.001). In multivariate analyses, compared to no discrimination, frequent healthcare discrimination was associated with new or worsened disability over 4 years (aHR = 1.63, 95 % CI 1.16-2.27).
Conclusions: One out of five adults over the age of 50 years experiences discrimination in healthcare settings. One in 17 experience frequent healthcare discrimination, and this is associated with new or worsened disability by 4 years. Future research should focus on the mechanisms by which healthcare discrimination influences disability in older adults to promote better health outcomes for an aging population.
Keywords: disability; discrimination; geriatrics.
Figures
Comment in
-
Knowing it When You See it: The Need for Continuing Innovation in Research on Healthcare Discrimination.J Gen Intern Med. 2015 Oct;30(10):1387-8. doi: 10.1007/s11606-015-3387-2. J Gen Intern Med. 2015. PMID: 25963584 Free PMC article. No abstract available.
References
-
- Stiefel M. Nolan. A Guide to Measuring the Triple Aim: Population Health, Experience of Care, and Per Capita Cost. IHI Innovation Series white paper. Cambridge: Institute for Healthcare Improvement; 2012.
-
- Anderson NB, Bulatao RA, Cohen B, National Research Council (US) Panel on Race E. Significance of Perceived Racism: Toward Understanding Ethnic Group Disparities in Health, the Later Years. 2004. http://www.ncbi.nlm.nih.gov/books/NBK25531/. Accessed December 5, 2013.
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
