

Outcomes of anatomical versus functional testing for coronary artery disease
- PMID: 25773919
- PMCID: PMC4473773
- DOI: 10.1056/NEJMoa1415516
Outcomes of anatomical versus functional testing for coronary artery disease
Abstract
Background: Many patients have symptoms suggestive of coronary artery disease (CAD) and are often evaluated with the use of diagnostic testing, although there are limited data from randomized trials to guide care.
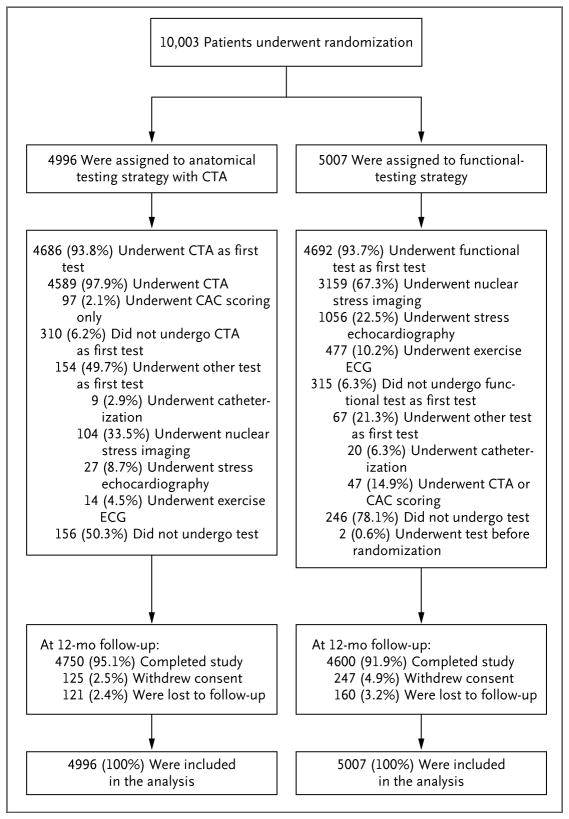
Methods: We randomly assigned 10,003 symptomatic patients to a strategy of initial anatomical testing with the use of coronary computed tomographic angiography (CTA) or to functional testing (exercise electrocardiography, nuclear stress testing, or stress echocardiography). The composite primary end point was death, myocardial infarction, hospitalization for unstable angina, or major procedural complication. Secondary end points included invasive cardiac catheterization that did not show obstructive CAD and radiation exposure.
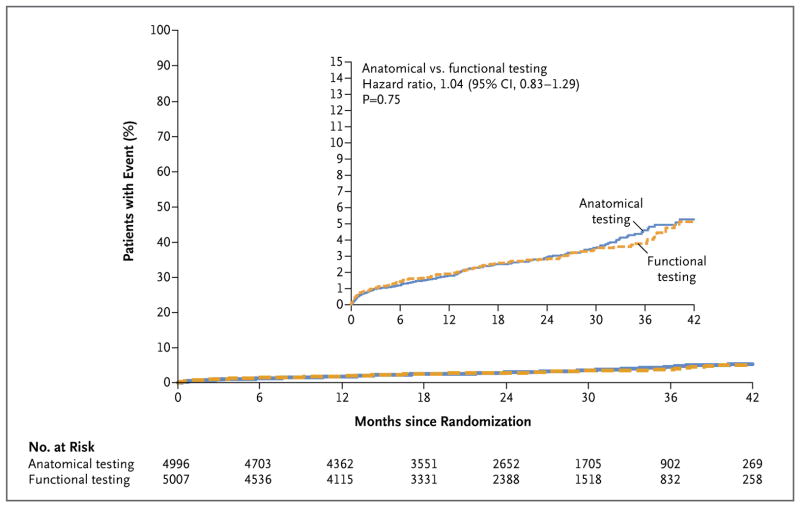
Results: The mean age of the patients was 60.8±8.3 years, 52.7% were women, and 87.7% had chest pain or dyspnea on exertion. The mean pretest likelihood of obstructive CAD was 53.3±21.4%. Over a median follow-up period of 25 months, a primary end-point event occurred in 164 of 4996 patients in the CTA group (3.3%) and in 151 of 5007 (3.0%) in the functional-testing group (adjusted hazard ratio, 1.04; 95% confidence interval, 0.83 to 1.29; P=0.75). CTA was associated with fewer catheterizations showing no obstructive CAD than was functional testing (3.4% vs. 4.3%, P=0.02), although more patients in the CTA group underwent catheterization within 90 days after randomization (12.2% vs. 8.1%). The median cumulative radiation exposure per patient was lower in the CTA group than in the functional-testing group (10.0 mSv vs. 11.3 mSv), but 32.6% of the patients in the functional-testing group had no exposure, so the overall exposure was higher in the CTA group (mean, 12.0 mSv vs. 10.1 mSv; P<0.001).
Conclusions: In symptomatic patients with suspected CAD who required noninvasive testing, a strategy of initial CTA, as compared with functional testing, did not improve clinical outcomes over a median follow-up of 2 years. (Funded by the National Heart, Lung, and Blood Institute; PROMISE ClinicalTrials.gov number, NCT01174550.).
Conflict of interest statement
No other potential conflict of interest relevant to this article was reported.
Figures
Comment in
-
Cardiovascular imaging and outcomes--PROMISEs to keep.N Engl J Med. 2015 Apr 2;372(14):1366-7. doi: 10.1056/NEJMe1501924. Epub 2015 Mar 14. N Engl J Med. 2015. PMID: 25773508 No abstract available.
-
[Which diagnostics should be used to clarify persistent, newly occurring cardiac complaints in outpatient treatment?].Radiologe. 2015 Jul;55(7):541-3. doi: 10.1007/s00117-015-2866-0. Radiologe. 2015. PMID: 26099593 German. No abstract available.
-
Anatomic and functional testing for coronary artery disease in symptomatic patients yield similar cardiovascular outcomes.Evid Based Med. 2015 Aug;20(4):145. doi: 10.1136/ebmed-2015-110212. Epub 2015 Jun 24. Evid Based Med. 2015. PMID: 26109577 No abstract available.
-
Anatomical versus Functional Testing for Coronary Artery Disease.N Engl J Med. 2015 Jul 2;373(1):91. doi: 10.1056/NEJMc1505594. N Engl J Med. 2015. PMID: 26132947 No abstract available.
-
Anatomical versus Functional Testing for Coronary Artery Disease.N Engl J Med. 2015 Jul 2;373(1):89. doi: 10.1056/NEJMc1505594. N Engl J Med. 2015. PMID: 26132948 No abstract available.
-
Anatomical versus Functional Testing for Coronary Artery Disease.N Engl J Med. 2015 Jul 2;373(1):89-90. doi: 10.1056/NEJMc1505594. N Engl J Med. 2015. PMID: 26132949 No abstract available.
-
Anatomical versus Functional Testing for Coronary Artery Disease.N Engl J Med. 2015 Jul 2;373(1):90. doi: 10.1056/NEJMc1505594. N Engl J Med. 2015. PMID: 26132950 No abstract available.
-
Anatomical versus Functional Testing for Coronary Artery Disease.N Engl J Med. 2015 Jul 2;373(1):90-1. doi: 10.1056/NEJMc1505594. N Engl J Med. 2015. PMID: 26132951 No abstract available.
-
ACP Journal Club: anatomical and functional testing did not differ for reducing CV events in suspected obstructive CAD.Ann Intern Med. 2015 Aug 18;163(4):JC11. doi: 10.7326/ACPJC-2015-163-4-011. Ann Intern Med. 2015. PMID: 26280433 No abstract available.
References
-
- Fihn SD, Gardin JM, Abrams J, et al. 2012 ACCF/AHA/ACP/AATS/PCNA/SCAI/STS Guideline for the diagnosis and management of patients with stable ischemic heart disease: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines, and the American College of Physicians, American Association for Thoracic Surgery, Preventive Cardiovascular Nurses Association, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons. J Am Coll Cardiol. 2012;60(24):e44–e164. - PubMed
-
- National Institute for Health and Care Excellence. Management of stable angina: NICE clinical guideline 126. 2012 Dec; http://www.nice.org.uk/guidance/cg126/resources/guidance-management-of-s.... - PubMed
-
- Montalescot G, Sechtem U, Achenbach S, et al. 2013 ESC guidelines on the management of stable coronary artery disease: the Task Force on the management of stable coronary artery disease of the European Society of Cardiology. Eur Heart J. 2013;34:2949–3003. - PubMed
-
- Rozanski A, Gransar H, Hayes SW, et al. Temporal trends in the frequency of inducible myocardial ischemia during cardiac stress testing: 1991 to 2009. J Am Coll Cardiol. 2013;61:1054–65. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous