

Repair of post-intubation tracheoesophageal fistulae through the left pre-sternocleidomastoid approach: a recent case series of 13 patients
- PMID: 25774303
- PMCID: PMC4332095
- DOI: 10.3978/j.issn.2072-1439.2015.02.01
Repair of post-intubation tracheoesophageal fistulae through the left pre-sternocleidomastoid approach: a recent case series of 13 patients
Abstract
Objective: Post-intubation tracheoesophageal fistula (TEF) is a late complication of tracheotomy, while membranous trachea laceration during percutaneous dilational tracheostomy is implicated in the generation of early post-tracheotomy TEF. Surgical repair is the only viable option for these patients and the technique of repair depends on a variety of factors.
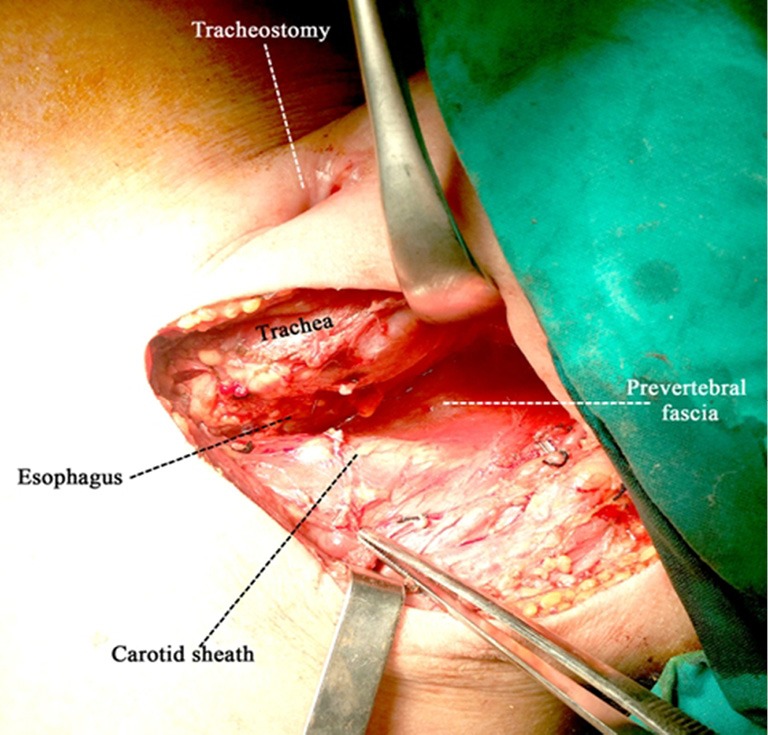
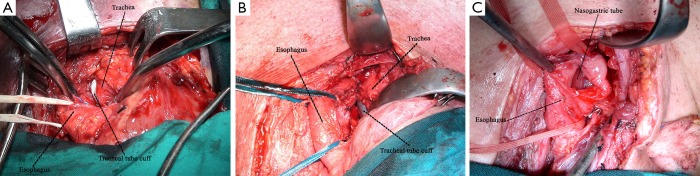
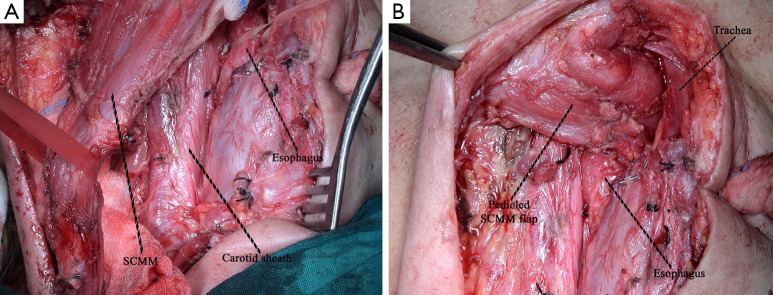
Methods: Totally 13 patients (mean age: 54.1±12.6 years; male: 8) with post-intubation TEF were managed between 2007 and 2013. The diagnosis was always made through esophagoscopy followed by endoscopic gastrostomy and bronchoscopy for repositioning of the tracheal tube just above the carina. Repair of the fistula was made in all patients through a left pre-sternocleidomastoid incision followed by dissection of the fistulous tract, suturing of esophagus and trachea and interposition of the whole pedicled left sternocleidomastoid muscle (SCMM) between the two suture lines.
Results: Five out of the 13 procedures were performed in mechanically ventilated patients; 3 of them died from septic complications during the postoperative period while fistula recurred in 1 of those 3 patients due to extensive inflammation of the tracheal wall. The rest 8 patients underwent fistula repair after weaning from mechanical ventilation and the results of repair were excellent. The additional procedure of temporary T-tube insertion was obviated in one patient to manage extensive tracheomalacia.
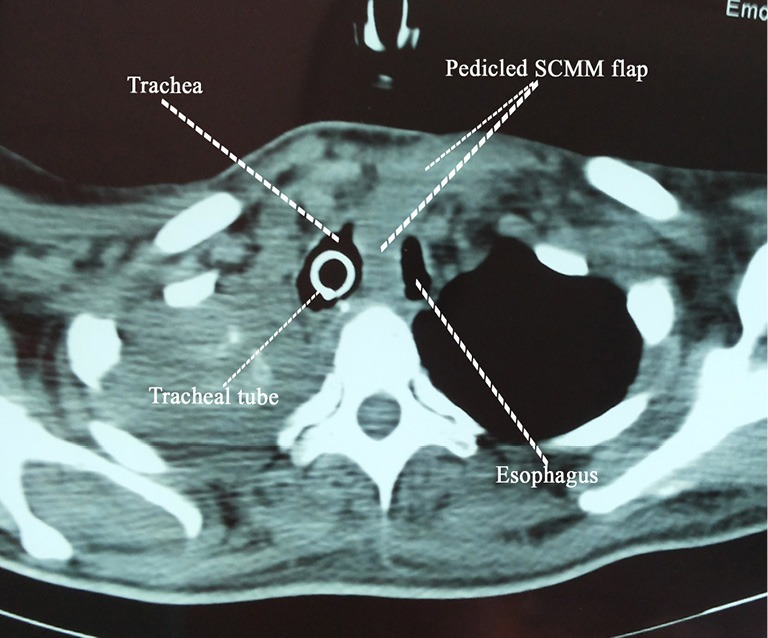
Conclusions: The left pre-sternocleidomastoid incision is an excellent access for the repair of a post-intubation TEF without tracheal resection. The interposition of the whole left pedicled SCMM between the suture lines of trachea and esophagus avoids fistula recurrence and offers the best chance for cure.
Keywords: Tracheoesophageal fistula (TEF); complications of tracheotomy; dilational tracheotomy; post-intubation tracheo-esophageal fistula; pre-sternocleidomastoid approach; tracheotomy.
Figures
Similar articles
-
Tracheoesophageal fistula.Chest Surg Clin N Am. 2003 May;13(2):271-89. doi: 10.1016/s1052-3359(03)00030-9. Chest Surg Clin N Am. 2003. PMID: 12755313 Review.
-
[Possibilities and results of surgical treatment of benign tracheoesophageal fistula].Rozhl Chir. 2010 Aug;89(8):478-89. Rozhl Chir. 2010. PMID: 21121142 Slovak.
-
Categorization and repair of recurrent and acquired tracheoesophageal fistulae occurring after esophageal atresia repair.J Pediatr Surg. 2017 Mar;52(3):424-430. doi: 10.1016/j.jpedsurg.2016.08.012. Epub 2016 Aug 31. J Pediatr Surg. 2017. PMID: 27616617
-
Stapled Repair of Benign Acquired Tracheoesophageal Fistula: Description of Novel Technique and Assessment of Outcomes.Cureus. 2020 Aug 18;12(8):e9854. doi: 10.7759/cureus.9854. Cureus. 2020. PMID: 32963896 Free PMC article.
-
Diagnosis and management of complete tracheal rings with concurrent tracheoesophageal fistula.Int J Pediatr Otorhinolaryngol. 2020 Jun;133:109971. doi: 10.1016/j.ijporl.2020.109971. Epub 2020 Feb 27. Int J Pediatr Otorhinolaryngol. 2020. PMID: 32179205
Cited by
-
Surgical Treatment Outcomes of Acquired Benign Tracheoesophageal Fistula: A Literature Review.J Chest Surg. 2021 Jun 5;54(3):206-213. doi: 10.5090/jcs.21.012. J Chest Surg. 2021. PMID: 33975983 Free PMC article.
-
Efficacy of mesenchymal stem cells in treating tracheoesophageal fistula via the TLR4/NF-κb pathway in beagle macrophages.Heliyon. 2024 Jun 13;10(12):e32903. doi: 10.1016/j.heliyon.2024.e32903. eCollection 2024 Jun 30. Heliyon. 2024. PMID: 39021940 Free PMC article.
-
Surgical repair of mechanical ventilation induced tracheoesophageal fistula.Eur Arch Otorhinolaryngol. 2020 Feb;277(2):323-331. doi: 10.1007/s00405-019-05723-y. Epub 2019 Nov 8. Eur Arch Otorhinolaryngol. 2020. PMID: 31705278 Review.
References
-
- Heffner JE, Miller KS, Sahn SA. Tracheostomy in the intensive care unit. Part 2: Complications. Chest 1986;90:430-6. - PubMed
-
- Epstein SK. Late complications of tracheostomy. Respir Care 2005;50:542-9. - PubMed
-
- De Leyn P, Bedert L, Delcroix M, et al. Tracheotomy: clinical review and guidelines. Eur J Cardiothorac Surg 2007;32:412-21. - PubMed
-
- Marzelle J, Dartevelle P, Khalife J, et al. Surgical management of acquired post-intubation tracheo-oesophageal fistulas: 27 patients. Eur J Cardiothorac Surg 1989;3:499-502; discussion 502-3. - PubMed
-
- Eleftheriadis E, Kotzampassi K.Temporary stenting of acquired benign tracheoesophageal fistulas in critically ill ventilated patients. Surg Endosc 2005;19:811-5. - PubMed
LinkOut - more resources
Full Text Sources