

Influence of Health Insurance Expansion on Disparities in the Treatment of Acute Cholecystitis
- PMID: 25775059
- PMCID: PMC4464963
- DOI: 10.1097/SLA.0000000000000970
Influence of Health Insurance Expansion on Disparities in the Treatment of Acute Cholecystitis
Abstract
Objective: To evaluate the impact of the 2006 Massachusetts (MA) health reform on disparities in the management of acute cholecystitis (AC).
Background: Immediate cholecystectomy has been shown to be the optimal treatment for AC, yet variation in care persists depending upon insurance status and patient race. How increased insurance coverage impacts these disparities in surgical care is not known.
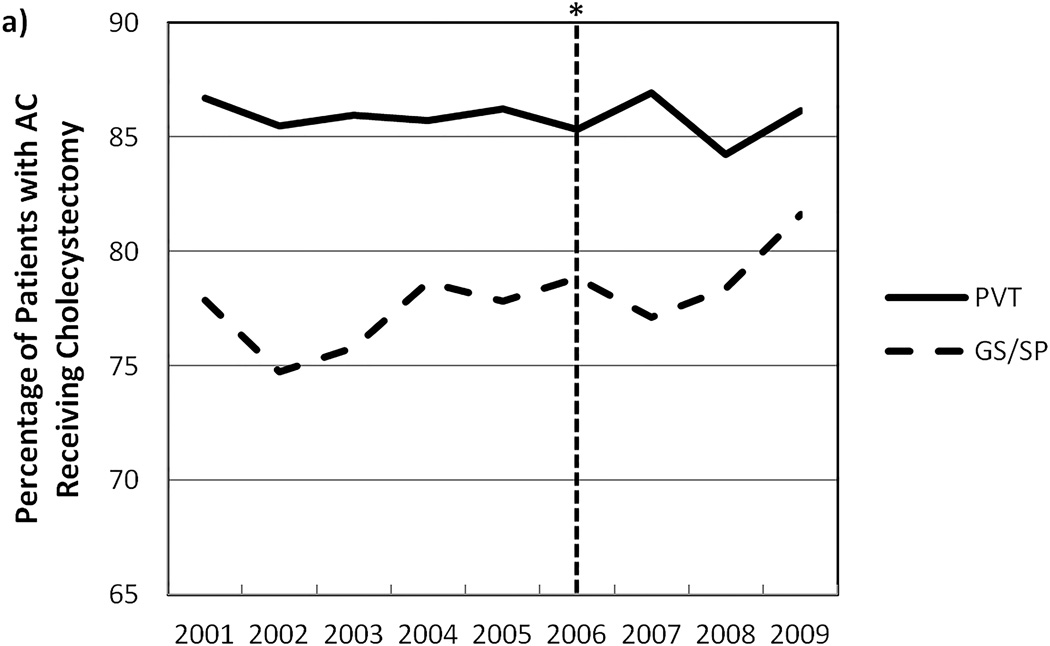
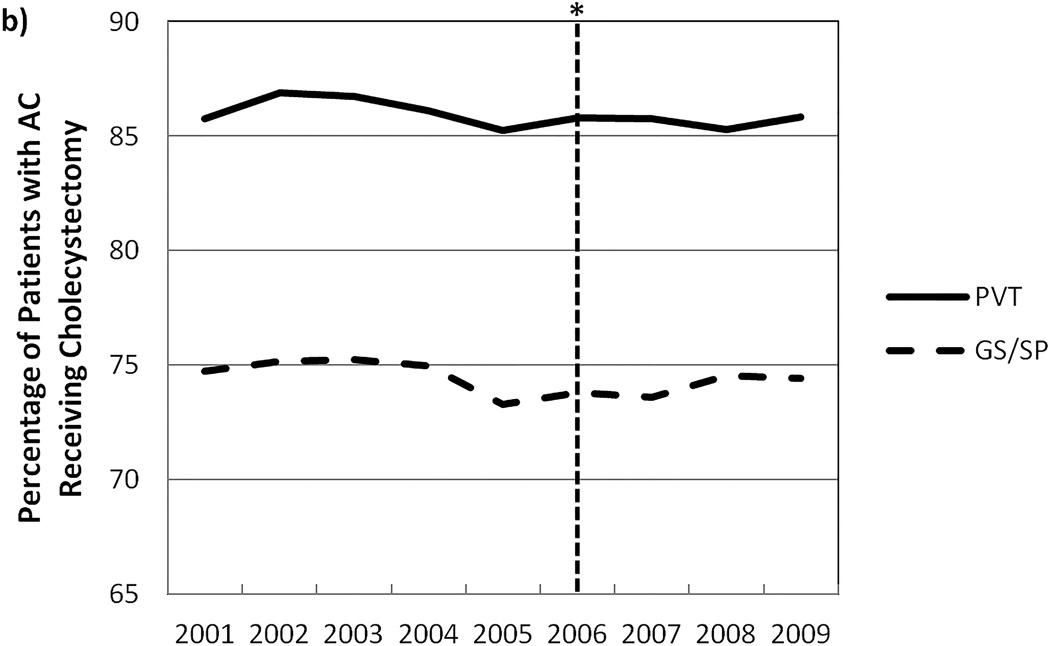
Methods: A cohort study of patients admitted with AC in MA and 3 control states from 2001 through 2009 was performed using the Hospital Cost and Utilization Project State Inpatient Databases. We examined all nonelderly white, black, or Latino patients by insurance type and patient race, evaluating changes in the probability of undergoing immediate cholecystectomy and disparities in receiving immediate cholecystectomy before and after Massachusetts health reform.
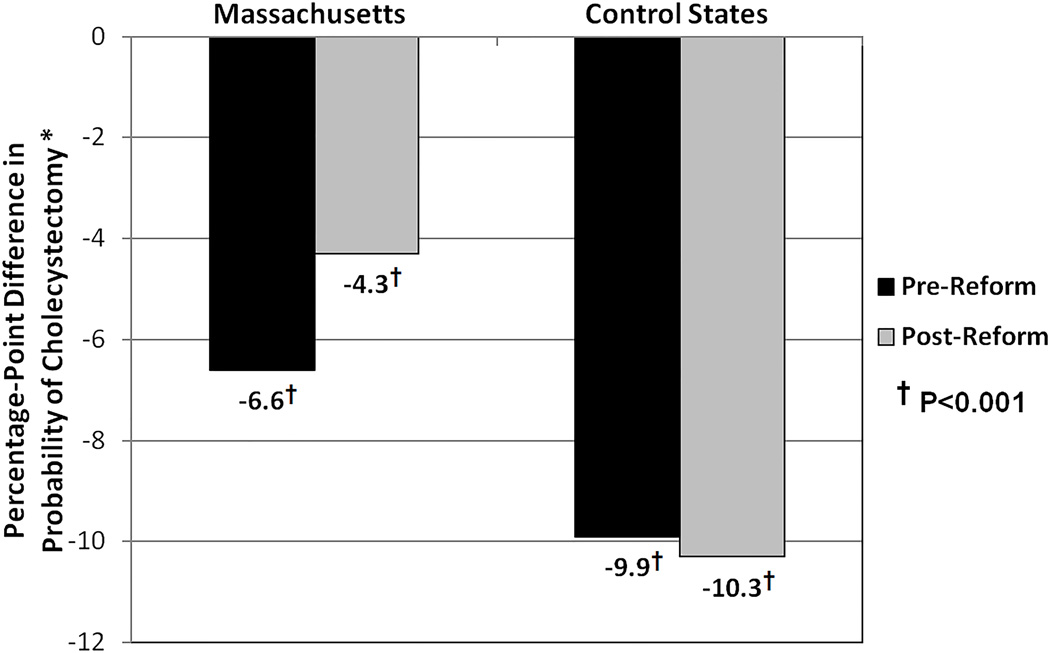
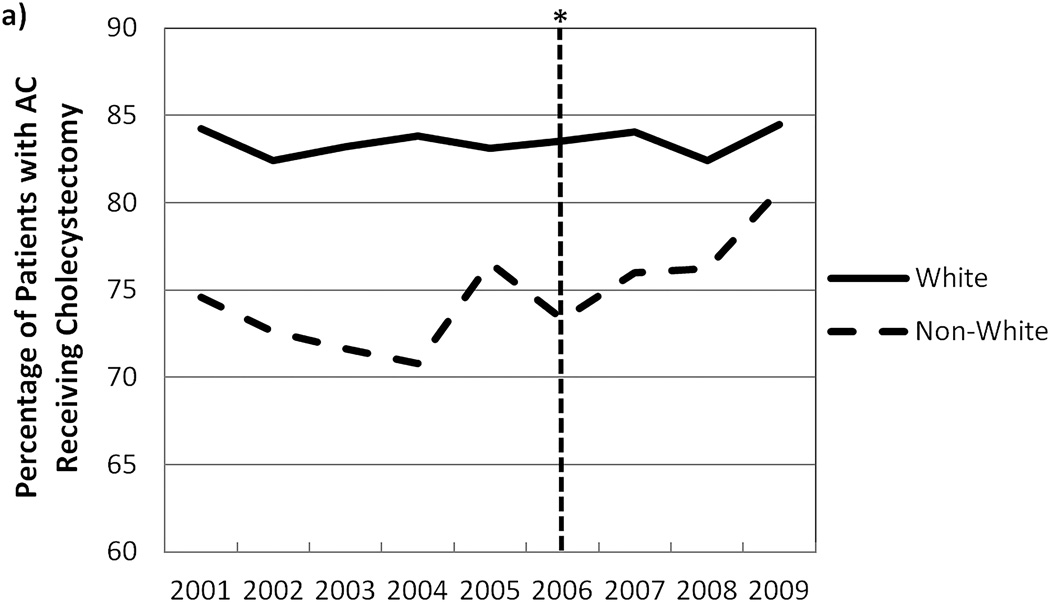
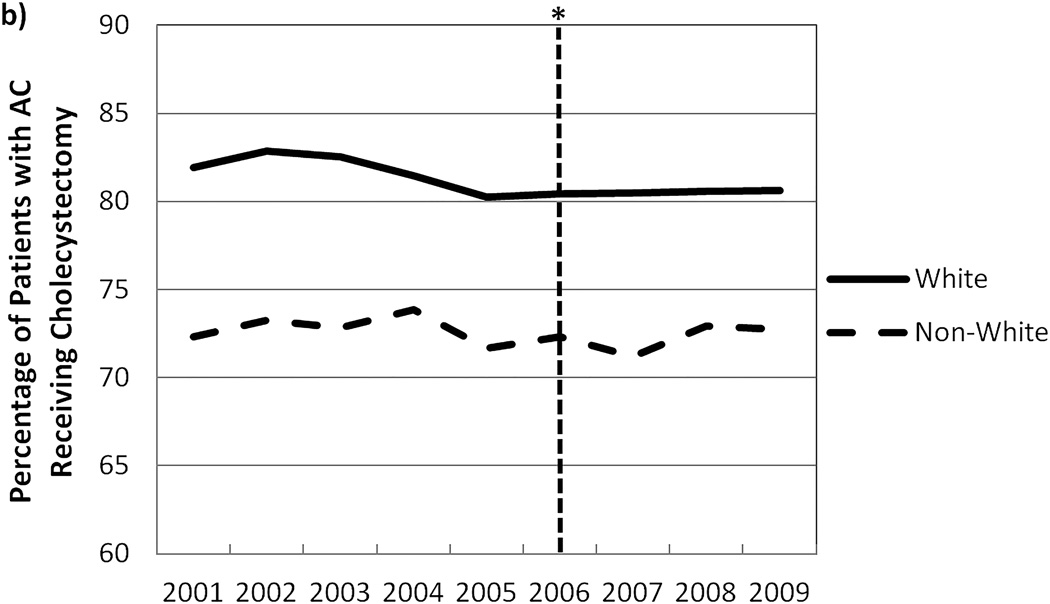
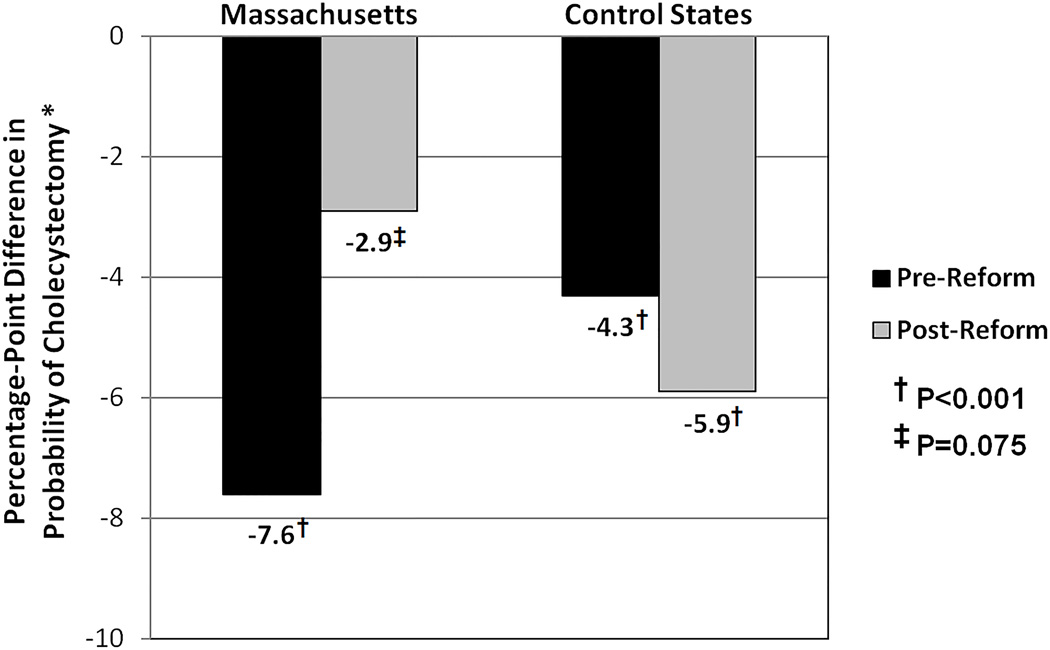
Results: Data from 141,344 patients hospitalized for AC were analyzed. Before the 2006 reform, government-subsidized/self-pay (GS/SP) patients had a 6.6 to 9.9 percentage-point lower (P < 0.001) probability of immediate cholecystectomy in both MA control states. The MA insurance expansion was independently associated with a 2.5 percentage-point increased probability of immediate cholecystectomy for all GS/SP patients in MA (P = 0.049) and a 5.0 percentage-point increased probability (P = 0.011) for nonwhite, GS/SP patients compared to control states. Racial disparities in the probability of immediate cholecystectomy seen before health care reform were no longer statistically significant after reform in MA while persisting in control states.
Conclusions: The MA health reform was associated with increased probability of undergoing immediate cholecystectomy for AC and reduced disparities in undergoing cholecystectomy by insurance status and patient race.
Figures
References
-
- Lidor AO, Gearhart SL, Wu AW, et al. Effect of race and insurance status on presentation, treatment and mortality in patients undergoing surgery for diverticulitis. Arch Surg. 2008;143:1160–1165. - PubMed
-
- Boston, MA: Division of Health Care Finance and Policy; 2010. [Accessed 13 May 2012]. Health Insurance Coverage in Massachusetts: Results from the 2008–2010 Massachusetts Health Insurance Surveys. Available at: http://www.mass.gov/chia/docs/r/pubs/10/mhis-report-12-2010.pdf.
-
- Long SK, Stockley K. Health Reform in Massachusetts: An update as of fall 2009. [Accessed 13 May 2012];Urban Institute. 2010 Available at: http://bluecrossmafoundation.org/~/media/Files/Publications/Policy%20Pub....
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
