

Immune activation response in chronic HIV-infected patients: influence of Hepatitis C virus coinfection
- PMID: 25775475
- PMCID: PMC4361597
- DOI: 10.1371/journal.pone.0119568
Immune activation response in chronic HIV-infected patients: influence of Hepatitis C virus coinfection
Abstract
Objectives: We have analyzed the parameters (bacterial translocation, immune activation and regulation, presence of HCV coinfection) which could be implicated in an inappropriate immune response from individuals with chronic HIV infection. The influence of them on the evolution of CD4+ T cell count has been investigated.
Patients and methods: Seventy HIV-infected patients [monoinfected by HIV (n = 20), HCV-coinfected (with (n = 25) and without (n = 25) liver cirrhosis)] and 25 healthy controls were included. Median duration of HIV infection was 20 years. HIV- and HCV-related parameters, as well as markers relative to bacterial translocation, monocyte and lymphocyte activation and regulation were considered as independent variables. Dependent variables were the increase of CD4+ T cell count during the follow-up (12 months).
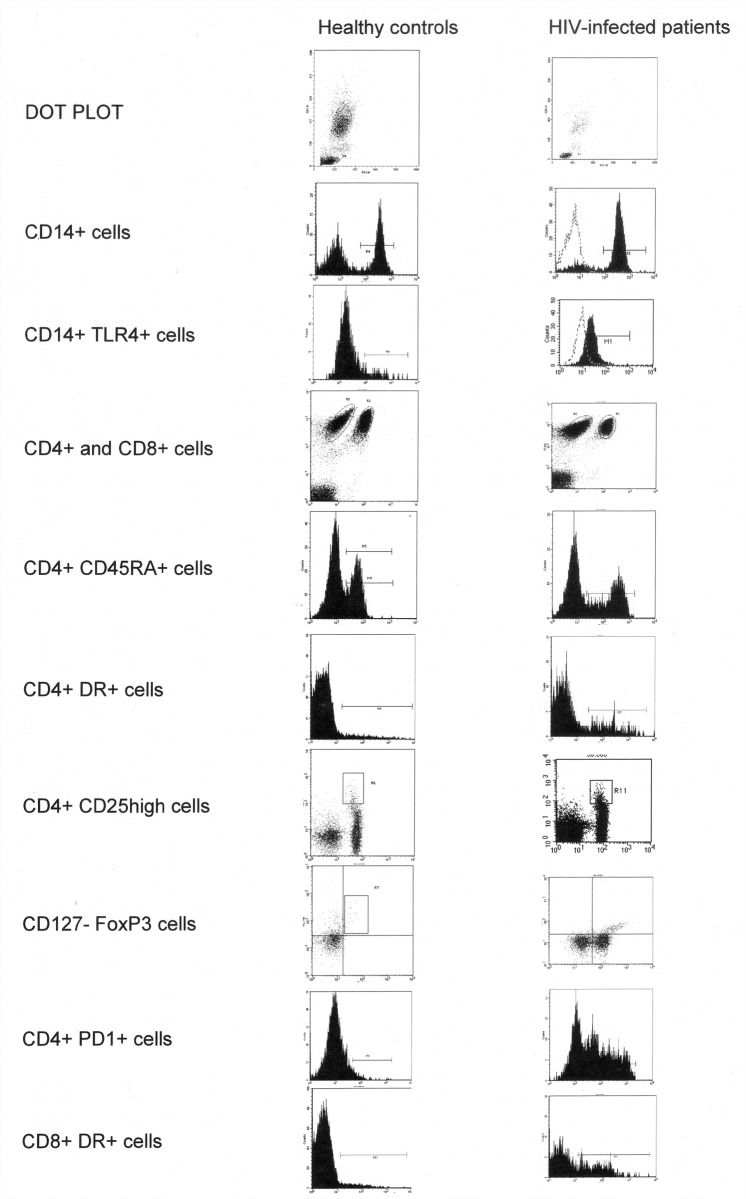
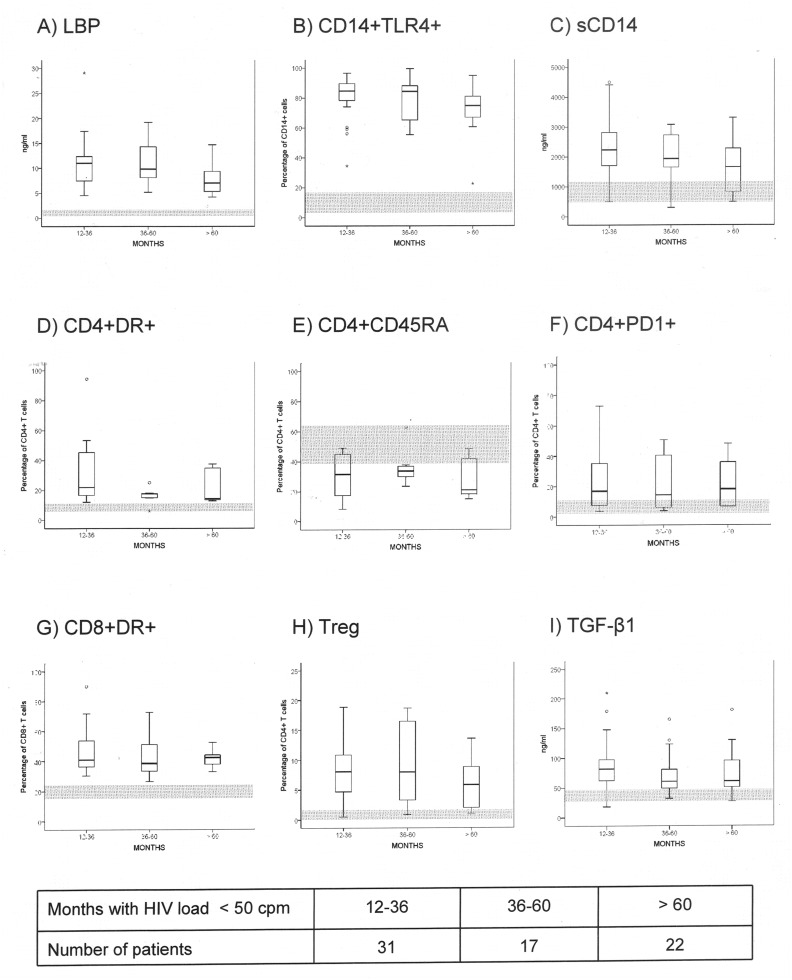
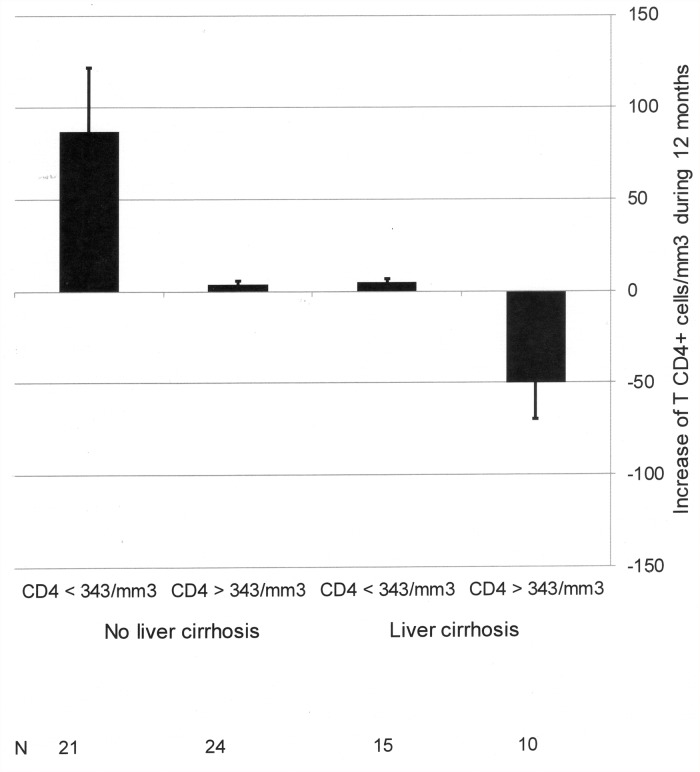
Results: Increased values of bacterial translocation, measured by lipopolysaccharide-binding protein, monocyte and lymphocyte activation markers and T regulatory lymphocytes were detected in HIV-monoinfected and HIV/HCV coinfected patients. Serum sCD14 and IL-6 were increased in HIV/HCV-coinfected patients with liver cirrhosis in comparison with those with chronic hepatitis or HIV-monoinfected individuals. Time with undetectable HIV load was not related with these parameters. The presence of cirrhosis was negatively associated with a CD4+ T cell count increase.
Conclusion: In patients with a chronic HIV infection, a persistent increase of lipopolysaccharide-binding protein and monocyte and lymphocyte modifications are present. HCV-related cirrhosis is associated with more elevated serum concentrations of monocyte-derived markers. Cirrhosis influences the continued immune reconstitution of these patients.
Conflict of interest statement
Figures
References
-
- DeHovitz JA, Kovacs A, Feldman JG, Anastos K, Young M, Cohen M, et al. The relationship between virus load response to highly active antiretroviral therapy and change in CD4 cell counts: A report from the Women’s Interagency HIV Study. J Infect Dis. 2000;182: 1527–1530. - PubMed
-
- Lange CG, Lederman MM. Immune reconstitution with antiretroviral therapies in chronic HIV-1 infection. J Antimicrob Chemother. 2003;51: 1–4. - PubMed
-
- Florence E, Lundgren J, Dreezen C, Fisher M, Kirk O, Blaxhult A, et al. Factors associated with a reduced CD4 lymphocyte count response to HAART despite full viral suppression in the EuroSIDA Study. HIV Med. 2003;4: 255–262. - PubMed
-
- Appay V, Sauce D. Immune activation and inflammation in HIV-1 infection: causes and consequences. J Pathol. 2008;214: 231–241. - PubMed
-
- Pitrak DL, Bolanos J, Hershow R, Novak RM. Discordant CD4 T lymphocyte responses to antiretroviral therapy for HIV infection are associated with ex-vivo rates of apoptosis. AIDS. 2001;15: 1317–1319. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
