

Disease activity in rheumatoid arthritis and the risk of cardiovascular events
- PMID: 25776112
- PMCID: PMC4446181
- DOI: 10.1002/art.39098
Disease activity in rheumatoid arthritis and the risk of cardiovascular events
Abstract
Objective: Use of several immunomodulatory agents has been associated with reduced numbers of cardiovascular (CV) events in epidemiologic studies of rheumatoid arthritis (RA). However, it is unknown whether time-averaged disease activity in RA correlates with CV events.
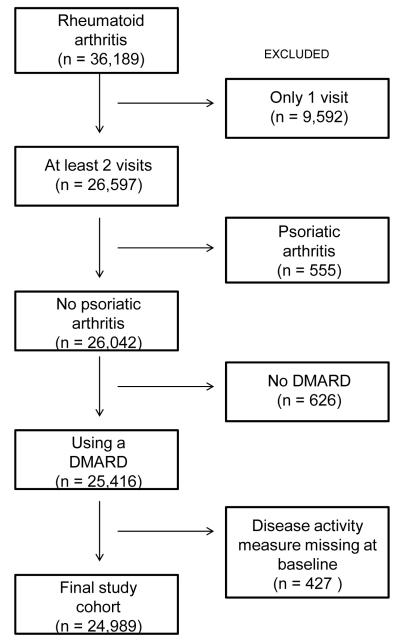
Methods: We studied patients with RA whose cases were followed in a longitudinal US-based registry. Time-averaged disease activity was assessed during followup using the area under the curve of the Clinical Disease Activity Index (CDAI), a validated measure of RA disease activity. Age, sex, presence of diabetes mellitus, hypertension, or hyperlipidemia, body mass index, family history of myocardial infarction (MI), use of aspirin or nonsteroidal antiinflammatory drugs (NSAIDs), presence of CV disease, and baseline use of an immunomodulator were assessed at baseline. Cox proportional hazards regression models were examined to determine the risk of a composite CV end point that included MI, stroke, and death from CV causes.
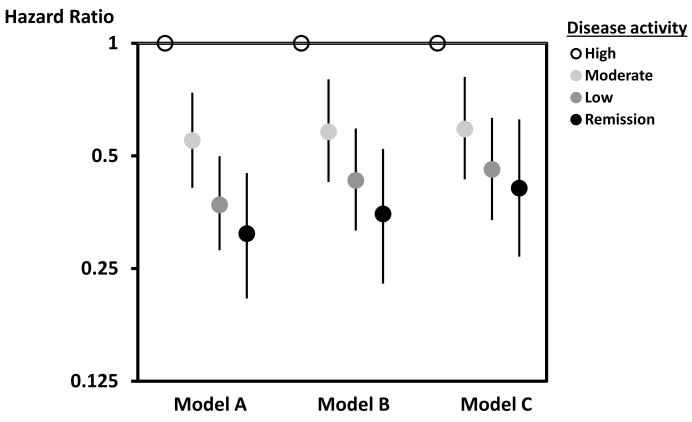
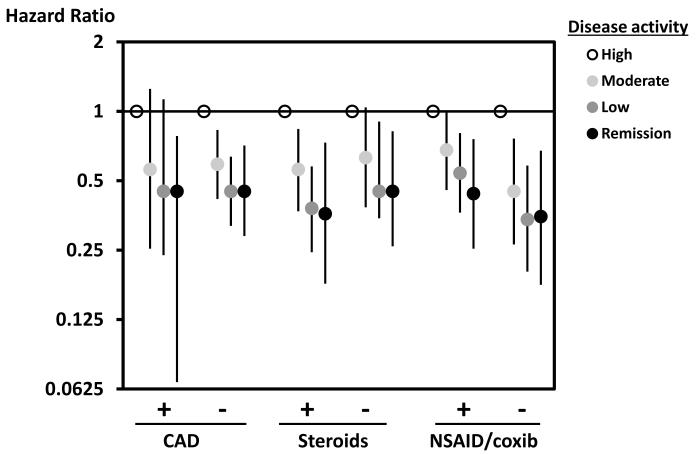
Results: A total of 24,989 patients who had been followed up for a median of 2.7 years were included in these analyses. During followup, we observed 534 confirmed CV end points, for an incidence rate of 7.8 per 1,000 person-years (95% confidence interval [95% CI] 6.7-8.9). In models adjusted for variables noted above, a 10-point reduction in the time-averaged CDAI was associated with a 21% reduction in CV risk (95% CI 13-29). These results were robust in subgroup analyses stratified by the presence of CV disease, use of corticosteroids, use of NSAIDs or selective cyclooxygenase 2 inhibitors, and change in RA treatment, as well as when restricted to events adjudicated as definite or probable.
Conclusion: Our findings showed that reduced time-averaged disease activity in RA is associated with fewer CV events.
© 2015, American College of Rheumatology.
Figures
References
-
- Avina-Zubieta JA, Choi HK, Sadatsafavi M, Etminan M, Esdaile JM, Lacaille D. Risk of cardiovascular mortality in patients with rheumatoid arthritis: a meta-analysis of observational studies. Arthritis Rheum. 2008;59(12):1690–7. - PubMed
-
- Solomon DH, Karlson EW, Rimm EB, Cannuscio CC, Mandl LA, Manson JE, et al. Cardiovascular morbidity and mortality in women diagnosed with rheumatoid arthritis.[see comment] Circulation. 2003;107(9):1303–7. - PubMed
-
- Del Rincon IWK, Stern MP, Freeman GL, O’Leary DH. Escalante A. Association between carotid atherosclerosis and markers of inflammation in rheumatoid arthritis patients and healthy subjects. Arthritis Rheum. 2002;48:1833–1840. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
