

Study for Updated Gout Classification Criteria: Identification of Features to Classify Gout
- PMID: 25777045
- PMCID: PMC4573373
- DOI: 10.1002/acr.22585
Study for Updated Gout Classification Criteria: Identification of Features to Classify Gout
Abstract
Objective: To determine which clinical, laboratory, and imaging features most accurately distinguished gout from non-gout.
Methods: We performed a cross-sectional study of consecutive rheumatology clinic patients with ≥1 swollen joint or subcutaneous tophus. Gout was defined by synovial fluid or tophus aspirate microscopy by certified examiners in all patients. The sample was randomly divided into a model development (two-thirds) and test sample (one-third). Univariate and multivariate association between clinical features and monosodium urate-defined gout was determined using logistic regression modeling. Shrinkage of regression weights was performed to prevent overfitting of the final model. Latent class analysis was conducted to identify patterns of joint involvement.
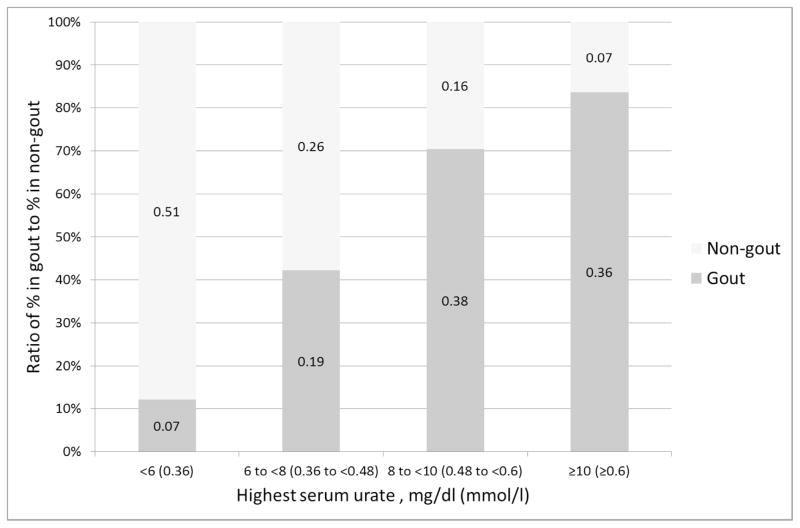
Results: In total, 983 patients were included. Gout was present in 509 (52%). In the development sample (n = 653), the following features were selected for the final model: joint erythema (multivariate odds ratio [OR] 2.13), difficulty walking (multivariate OR 7.34), time to maximal pain <24 hours (multivariate OR 1.32), resolution by 2 weeks (multivariate OR 3.58), tophus (multivariate OR 7.29), first metatarsophalangeal (MTP1) joint ever involved (multivariate OR 2.30), location of currently tender joints in other foot/ankle (multivariate OR 2.28) or MTP1 joint (multivariate OR 2.82), serum urate level >6 mg/dl (0.36 mmoles/liter; multivariate OR 3.35), ultrasound double contour sign (multivariate OR 7.23), and radiograph erosion or cyst (multivariate OR 2.49). The final model performed adequately in the test set, with no evidence of misfit, high discrimination, and predictive ability. MTP1 joint involvement was the most common joint pattern (39.4%) in gout cases.
Conclusion: Ten key discriminating features have been identified for further evaluation for new gout classification criteria. Ultrasound findings and degree of uricemia add discriminating value, and will significantly contribute to more accurate classification criteria.
© 2015, American College of Rheumatology.
Figures
References
-
- Neogi T. Clinical practice. Gout N Engl J Med. 2011;364(5):443–52. - PubMed
-
- Trifiro G, Morabito P, Cavagna L, Ferrajolo C, Pecchioli S, Simonetti M, et al. Epidemiology of gout and hyperuricaemia in Italy during the years 2005–2009: a nationwide population-based study. Ann Rheum Dis. 2013;72(5):694–700. - PubMed
-
- Wallace SL, Robinson H, Masi AT, Decker JL, McCarty DJ, Yu TF. Preliminary criteria for the classification of the acute arthritis of primary gout. Arthritis Rheum. 1977;20(3):895–900. - PubMed
-
- Malik A, Schumacher HR, Dinnella JE, Clayburne GM. Clinical diagnostic criteria for gout: comparison with the gold standard of synovial fluid crystal analysis. JCR: Journal of Clinical Rheumatology. 2009;15(1):22–4. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
