

Mood Disorders in Systemic Lupus Erythematosus: Results From an International Inception Cohort Study
- PMID: 25778456
- PMCID: PMC4485527
- DOI: 10.1002/art.39111
Mood Disorders in Systemic Lupus Erythematosus: Results From an International Inception Cohort Study
Abstract
Objective: To examine the frequency, characteristics, and outcome of mood disorders, as well as clinical and autoantibody associations, in a multiethnic/racial, prospective inception cohort of patients with systemic lupus erythematosus (SLE).
Methods: Patients were assessed annually for mood disorders (4 types, according to the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition) and 18 other neuropsychiatric events. Global disease activity scores (SLE Disease Activity Index 2000 [SLEDAI-2K]), damage scores (Systemic Lupus International Collaborating Clinics/American College of Rheumatology Damage Index [SDI]), and Short Form 36 subscales, mental and physical component summary scores were collected. Time to event, linear and ordinal regressions, and multi-state models were used as appropriate.
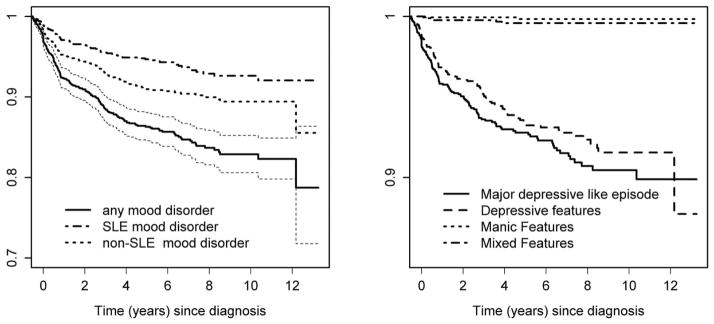
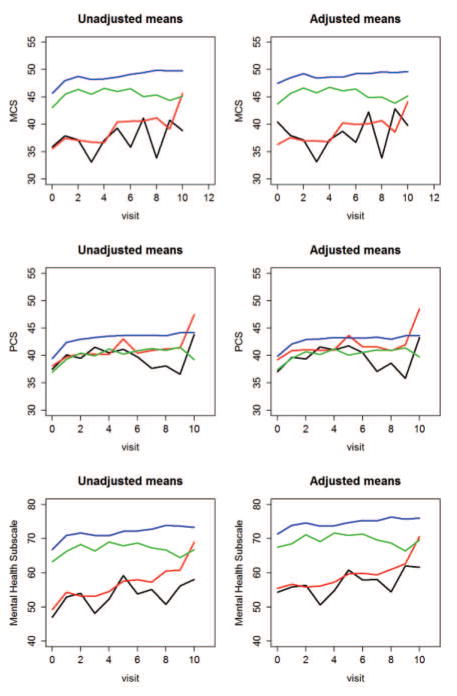
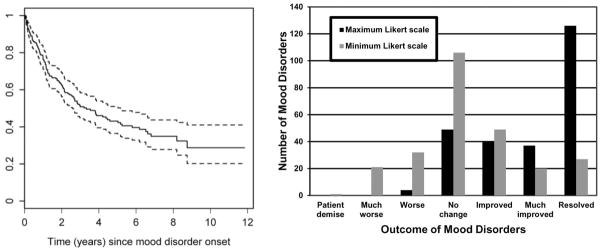
Results: Among the 1,827 patients with SLE, 88.9% were female, and 48.9% were Caucasian. The mean ± SD age of the patients was 35.1 ± 13.3 years, disease duration was 5.6 ± 4.8 months, and the length of followup was 4.7 ± 3.5 years. During the course of the study, 863 (47.2%) of the 1,827 patients had 1,627 neuropsychiatric events. Mood disorders occurred in 232 (12.7%) of 1,827 patients, and 98 (38.3%) of 256 mood disorder events were attributed to SLE. The estimated cumulative incidence of any mood disorder after 10 years was 17.7% (95% confidence interval 15.1, 20.2%). A greater risk of mood disorder was associated with concurrent neuropsychiatric events (P ≤ 0.01), and a lower risk was associated with Asian race/ethnicity (P = 0.01) and treatment with immunosuppressive drugs (P = 0.003). Mood disorders were associated with lower mental health and mental component summary scores but not with the SLEDAI-2K, SDI, or lupus autoantibodies. Among the 232 patients with depression, 168 (72.4%) were treated with antidepressants. One hundred twenty-six (49.2%) of 256 mood disorders resolved in 117 (50.4%) of 232 patients.
Conclusion: Mood disorders, the second most frequent neuropsychiatric event in patients with SLE, have a negative impact on health-related quality of life and improve over time. The lack of association with global SLE disease activity, cumulative organ damage, and lupus autoantibodies emphasizes the multifactorial etiology of mood disorders and a role for non-lupus-specific therapies.
© 2015, American College of Rheumatology.
Figures
References
-
- Ainiala H, Loukkola J, Peltola J, Korpela M, Hietaharju A. The prevalence of neuropsychiatric syndromes in systemic lupus erythematosus. Neurology. 2001;57(3):496–500. - PubMed
-
- Brey RL, Holliday SL, Saklad AR, Navarrete MG, Hermosillo-Romo D, Stallworth CL, et al. Neuropsychiatric syndromes in lupus: prevalence using standardized definitions. Neurology. 2002;58(8):1214–20. - PubMed
-
- Hanly JG, McCurdy G, Fougere L, Douglas JA, Thompson K. Neuropsychiatric events in systemic lupus erythematosus: attribution and clinical significance. J Rheumatol. 2004;31(11):2156–62. - PubMed
-
- Sanna G, Bertolaccini ML, Cuadrado MJ, Laing H, Mathieu A, Hughes GR. Neuropsychiatric manifestations in systemic lupus erythematosus: prevalence and association with antiphospholipid antibodies. J Rheumatol. 2003;30(5):985–92. - PubMed
-
- Sibbitt WL, Jr, Brandt JR, Johnson CR, Maldonado ME, Patel SR, Ford CC, et al. The incidence and prevalence of neuropsychiatric syndromes in pediatric onset systemic lupus erythematosus. J Rheumatol. 2002;29(7):1536–42. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- K24-AR-2318/AR/NIAMS NIH HHS/United States
- MOP-86526/CAPMC/ CIHR/Canada
- UL1 RR025741/RR/NCRR NIH HHS/United States
- RR-00046/RR/NCRR NIH HHS/United States
- P60-AR-4464/AR/NIAMS NIH HHS/United States
- 8-UL-1TR-000150/TR/NCATS NIH HHS/United States
- AR-43727/AR/NIAMS NIH HHS/United States
- MC_U105261167/MRC_/Medical Research Council/United Kingdom
- M01 RR000046/RR/NCRR NIH HHS/United States
- UL-1RR-025741/RR/NCRR NIH HHS/United States
- P60-AR-8098/AR/NIAMS NIH HHS/United States
- UL1 TR000150/TR/NCATS NIH HHS/United States
- P60 AR064464/AR/NIAMS NIH HHS/United States
- P60 AR048098/AR/NIAMS NIH HHS/United States
- MR/K00414X/1/MRC_/Medical Research Council/United Kingdom
- U105261167/MRC_/Medical Research Council/United Kingdom
- R01 AR043727/AR/NIAMS NIH HHS/United States
- ARC_/Arthritis Research UK/United Kingdom
- K24 AR002138/AR/NIAMS NIH HHS/United States
- WT_/Wellcome Trust/United Kingdom
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
