

AIDS incidence and AIDS-related mortality in British Columbia, Canada, between 1981 and 2013: a retrospective study
- PMID: 25780802
- PMCID: PMC4357843
- DOI: 10.1016/S2352-3018(15)00017-X
AIDS incidence and AIDS-related mortality in British Columbia, Canada, between 1981 and 2013: a retrospective study
Abstract
Background: Appropriate use of highly active antiretroviral therapy (ART) can substantially decrease the risk of progression to AIDS and of premature mortality. We aimed to characterise the trends between 1981 and 2013 in AIDS-defining illnesses (ADIs) and the number AIDS-related deaths in British Columbia, Canada, where ART has been fully subsidised since 1996.
Methods: We included data on HIV-positive individuals, aged 19 years or older, from four administrative databases in British Columbia: the British Columbia Centre for Excellence in HIV/AIDS, St Paul's Hospital, the British Columbia Vital Statistics Agency, the British Columbia Cancer Agency. We estimated the relative risk of developing an ADI over time by use of a negative binomial model, and we investigated trends in the proportion of all deaths associated with AIDS by use of generalised additive models.
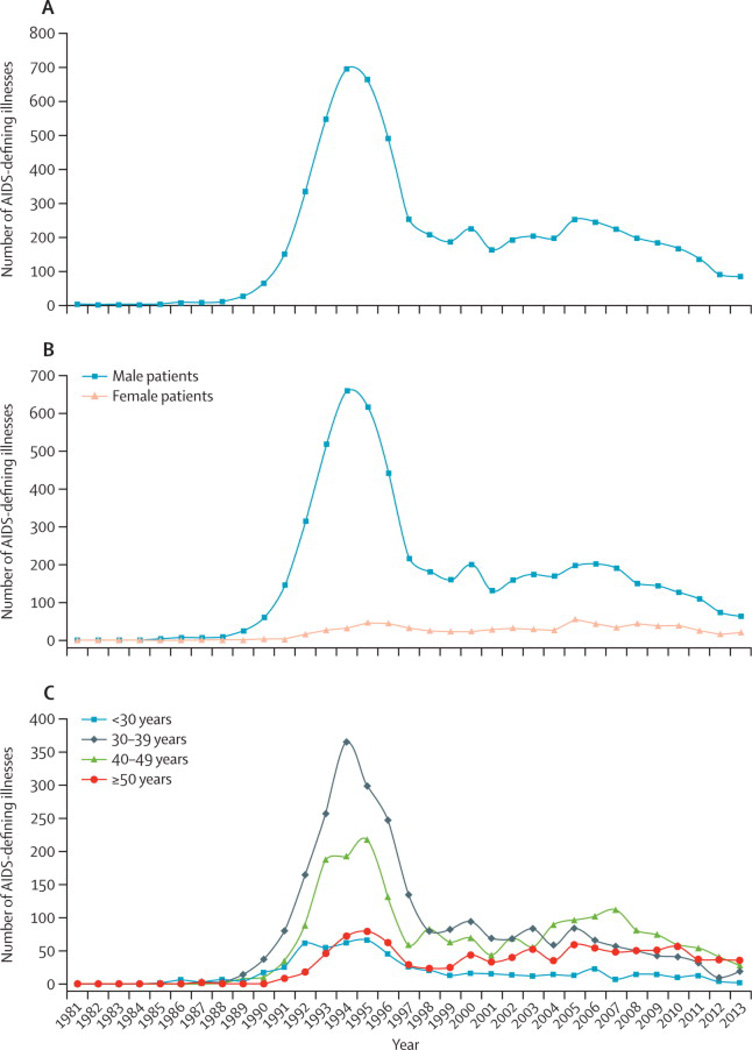
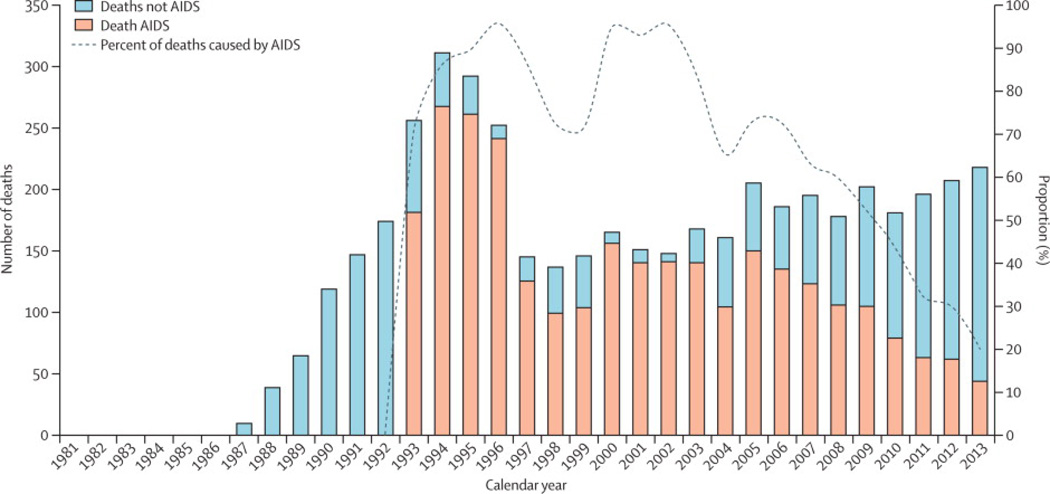
Findings: Data were available for 3550 people with HIV. 6205 ADIs were recorded. In 2013, 84 ADIs occurred, the lowest number since 1990. The peak of the AIDS epidemic in the region happened in 1994 with 696 ADIs reported (42 ADIs per 100 person-years). Since 1997, the number of ADIs decreased from 253 (7 per 100 person-years) to 84 cases in 2013 (1 per 100 person-years; p<0·0001 for trend in number of ADIs). We have also shown that of 22 ADIs included, only Pneumocystis jirovecii pneumonia remained prominent (albeit with much reduced overall prevalence). 2828 deaths were from AIDS-related causes, peaking in 1996 with 241 (96%) of 252 deaths in people with HIV and declining to 44 (20%) of 218 in 2013.
Interpretation: Our results provide further evidence that integrated comprehensive free programmes that facilitate testing and deliver treatment and care can be eff ective in decreasing AIDS-related morbidity and mortality, thus suggesting that control of and eventually an end to AIDS are possible.
Conflict of interest statement
We have the following conflicts of interest: JSGM has received limited unrestricted funding, paid to his institution, from Abbvie, Bristol-Myers Squibb, Gilead Sciences, Janssen, Merck, and ViiV Healthcare. VDL has received limited unrestricted funding, paid to her institution, from GlaxoSmithKline. The remaining authors do not have conflicts to declare.
Figures
Comment in
-
End of AIDS on the horizon, but innovation needed to end HIV.Lancet HIV. 2015 Mar;2(3):e74-5. doi: 10.1016/S2352-3018(15)00023-5. Epub 2015 Feb 13. Lancet HIV. 2015. PMID: 26424545 No abstract available.
References
-
- Carpenter CC, Fischl MA, Hammer SM, et al. Antiretroviral therapy for HIV infection in 1996. Recommendations of an international panel. International AIDS Society-USA. JAMA : the journal of the American Medical Association. 1996;276(2):146–154. - PubMed
-
- Thompson MA, Aberg JA, Hoy JF, et al. Antiretroviral treatment of adult HIV infection: 2012 recommendations of the International Antiviral Society-USA panel. JAMA : the journal of the American Medical Association. 2012;308(4):387–402. - PubMed
-
- Joint United Nations Programme on HIV/AIDS (UNAIDS) Global report: UNAIDS report on the global AIDS epidemic 2013 [Online] Geneva: UNAIDS; 2013. [cited 2014 September 1]. [updated 2013 November;]. Available from: http://www.unaids.org/en/media/unaids/contentassets/documents/epidemiolo....
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
