

Diagnostic concordance among pathologists interpreting breast biopsy specimens
- PMID: 25781441
- PMCID: PMC4516388
- DOI: 10.1001/jama.2015.1405
Diagnostic concordance among pathologists interpreting breast biopsy specimens
Abstract
Importance: A breast pathology diagnosis provides the basis for clinical treatment and management decisions; however, its accuracy is inadequately understood.
Objectives: To quantify the magnitude of diagnostic disagreement among pathologists compared with a consensus panel reference diagnosis and to evaluate associated patient and pathologist characteristics.
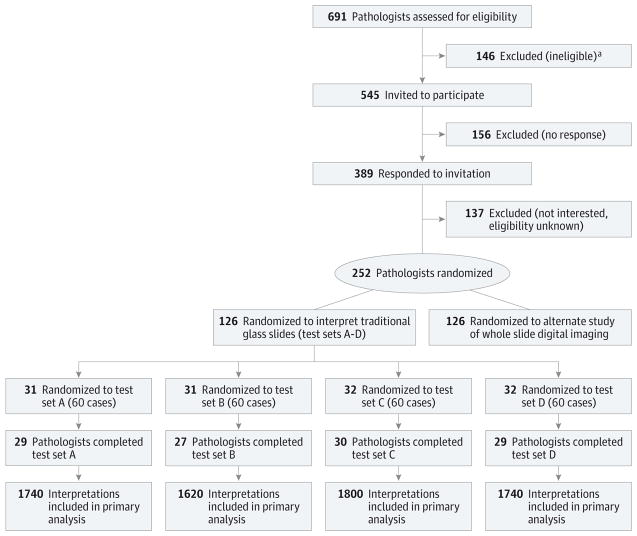
Design, setting, and participants: Study of pathologists who interpret breast biopsies in clinical practices in 8 US states.
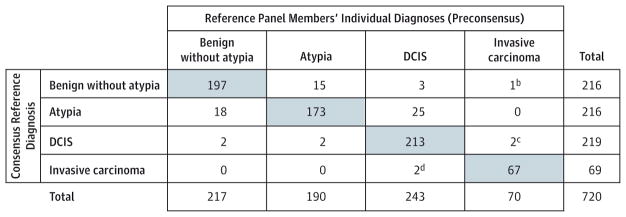
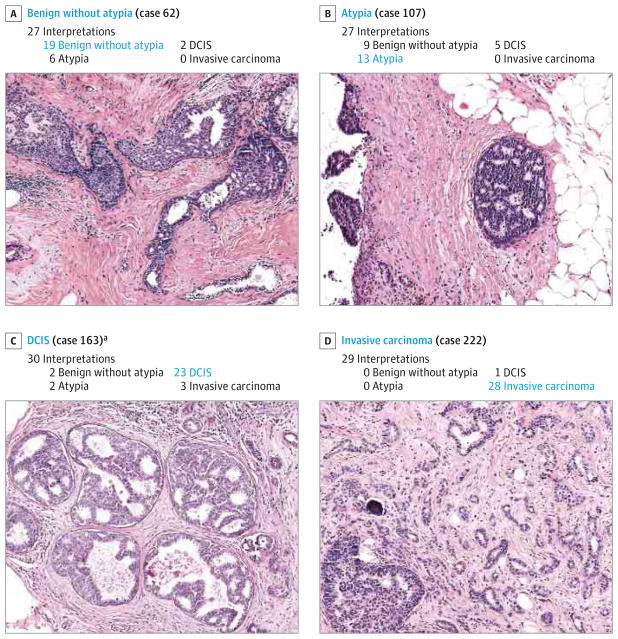
Exposures: Participants independently interpreted slides between November 2011 and May 2014 from test sets of 60 breast biopsies (240 total cases, 1 slide per case), including 23 cases of invasive breast cancer, 73 ductal carcinoma in situ (DCIS), 72 with atypical hyperplasia (atypia), and 72 benign cases without atypia. Participants were blinded to the interpretations of other study pathologists and consensus panel members. Among the 3 consensus panel members, unanimous agreement of their independent diagnoses was 75%, and concordance with the consensus-derived reference diagnoses was 90.3%.
Main outcomes and measures: The proportions of diagnoses overinterpreted and underinterpreted relative to the consensus-derived reference diagnoses were assessed.
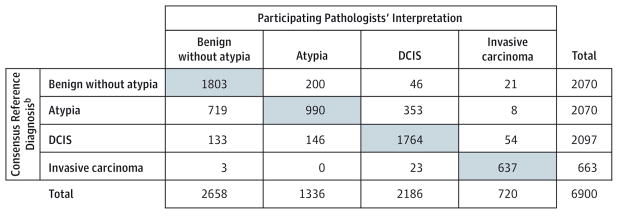
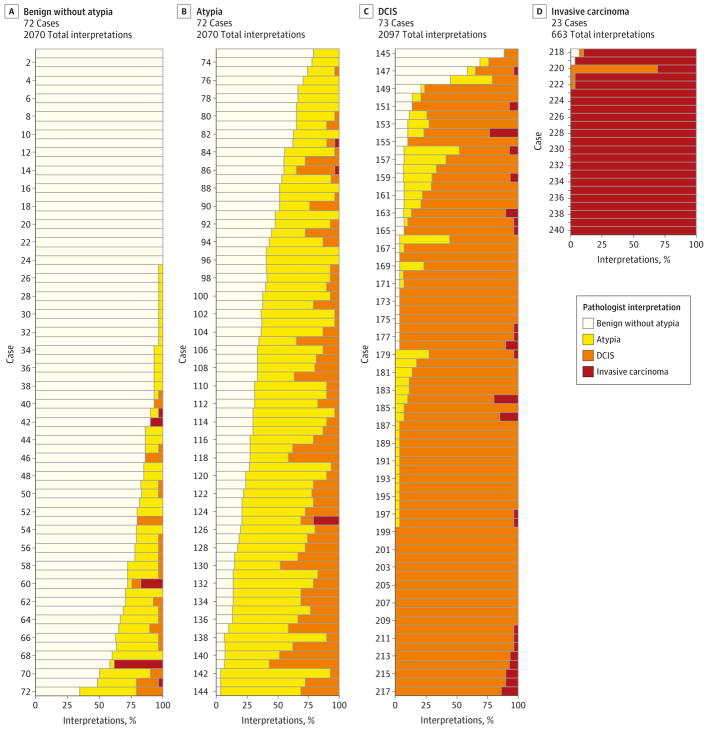
Results: Sixty-five percent of invited, responding pathologists were eligible and consented to participate. Of these, 91% (N = 115) completed the study, providing 6900 individual case diagnoses. Compared with the consensus-derived reference diagnosis, the overall concordance rate of diagnostic interpretations of participating pathologists was 75.3% (95% CI, 73.4%-77.0%; 5194 of 6900 interpretations). Among invasive carcinoma cases (663 interpretations), 96% (95% CI, 94%-97%) were concordant, and 4% (95% CI, 3%-6%) were underinterpreted; among DCIS cases (2097 interpretations), 84% (95% CI, 82%-86%) were concordant, 3% (95% CI, 2%-4%) were overinterpreted, and 13% (95% CI, 12%-15%) were underinterpreted; among atypia cases (2070 interpretations), 48% (95% CI, 44%-52%) were concordant, 17% (95% CI, 15%-21%) were overinterpreted, and 35% (95% CI, 31%-39%) were underinterpreted; and among benign cases without atypia (2070 interpretations), 87% (95% CI, 85%-89%) were concordant and 13% (95% CI, 11%-15%) were overinterpreted. Disagreement with the reference diagnosis was statistically significantly higher among biopsies from women with higher (n = 122) vs lower (n = 118) breast density on prior mammograms (overall concordance rate, 73% [95% CI, 71%-75%] for higher vs 77% [95% CI, 75%-80%] for lower, P < .001), and among pathologists who interpreted lower weekly case volumes (P < .001) or worked in smaller practices (P = .034) or nonacademic settings (P = .007).
Conclusions and relevance: In this study of pathologists, in which diagnostic interpretation was based on a single breast biopsy slide, overall agreement between the individual pathologists' interpretations and the expert consensus-derived reference diagnoses was 75.3%, with the highest level of concordance for invasive carcinoma and lower levels of concordance for DCIS and atypia. Further research is needed to understand the relationship of these findings with patient management.
Conflict of interest statement
Figures
Comment in
-
Expertise vs evidence in assessment of breast biopsies: an atypical science.JAMA. 2015 Mar 17;313(11):1109-10. doi: 10.1001/jama.2015.1945. JAMA. 2015. PMID: 25781438 No abstract available.
-
Minimizing Errors in Breast Pathology: A Call for Action.Breast J. 2015 Jul-Aug;21(4):333-6. doi: 10.1111/tbj.12440. Breast J. 2015. PMID: 26136182 No abstract available.
-
Discordant Interpretations of Breast Biopsy Specimens by Pathologists.JAMA. 2015 Jul 7;314(1):82-3. doi: 10.1001/jama.2015.6224. JAMA. 2015. PMID: 26151272 No abstract available.
-
Discordant Interpretations of Breast Biopsy Specimens by Pathologists.JAMA. 2015 Jul 7;314(1):82. doi: 10.1001/jama.2015.6230. JAMA. 2015. PMID: 26151273 No abstract available.
-
Discordant Interpretations of Breast Biopsy Specimens by Pathologists--Reply.JAMA. 2015 Jul 7;314(1):83-4. doi: 10.1001/jama.2015.6239. JAMA. 2015. PMID: 26151274 No abstract available.
References
-
- Silverstein M. Where’s the outrage? J Am Coll Surg. 2009;208(1):78–79. - PubMed
-
- Silverstein MJ, Recht A, Lagios MD, et al. Special report: Consensus conference III: image-detected breast cancer: state-of-the-art diagnosis and treatment [published correction appears in J Am Coll Surg. 2009 Dec;209(6):802] J Am Coll Surg. 2009;209(4):504–520. - PubMed
-
- Weaver DL, Rosenberg RD, Barlow WE, et al. Pathologic findings from the Breast Cancer Surveillance Consortium: population-based outcomes in women undergoing biopsy after screening mammography. Cancer. 2006;106(4):732–742. - PubMed
-
- Harris JR, Lippman ME, Morrow M, Osborne CK. Diseases of the Breast. 5. Philadelphia, PA: Wolters Kluwer Health; 2014.
-
- Bleyer A, Welch HG. Effect of 3 decades of screening mammography on breast-cancer incidence. N Engl J Med. 2012;367(21):1998–2005. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
