

Incremental benefits of screening colonoscopy over sigmoidoscopy in average-risk populations: a model-driven analysis
- PMID: 25783458
- PMCID: PMC4646080
- DOI: 10.1007/s10552-015-0559-7
Incremental benefits of screening colonoscopy over sigmoidoscopy in average-risk populations: a model-driven analysis
Abstract
Purpose: Screening colonoscopy and flexible sigmoidoscopy (FSG) reduce the risk of colorectal cancer (CRC), but the magnitude and duration of protection, particularly against right-sided cancer, remain uncertain. We computed the incremental benefit of colonoscopy over FSG using a validated mathematical model, which reflects colorectal neoplasia growth characteristics while allowing uncertainty in endoscopic detection and removal of adenomas.
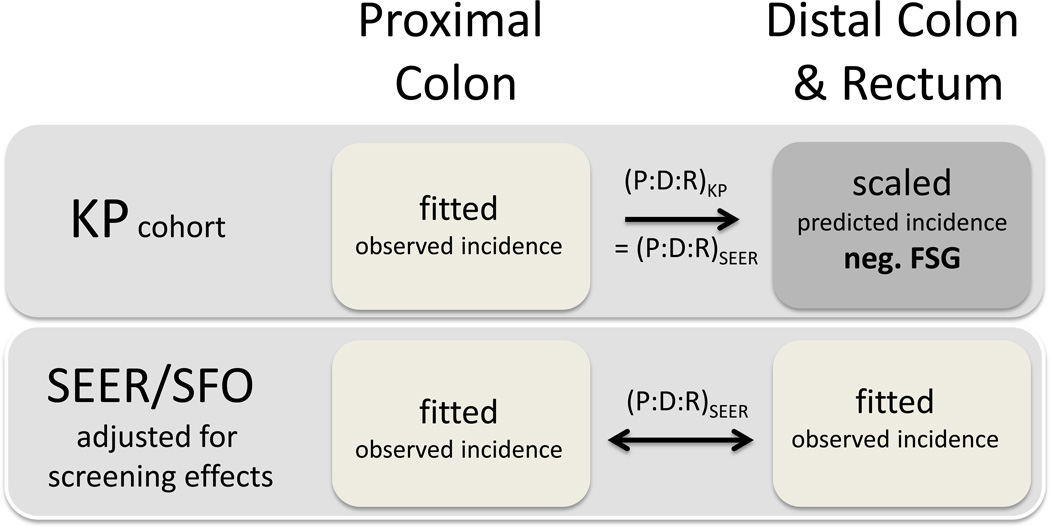
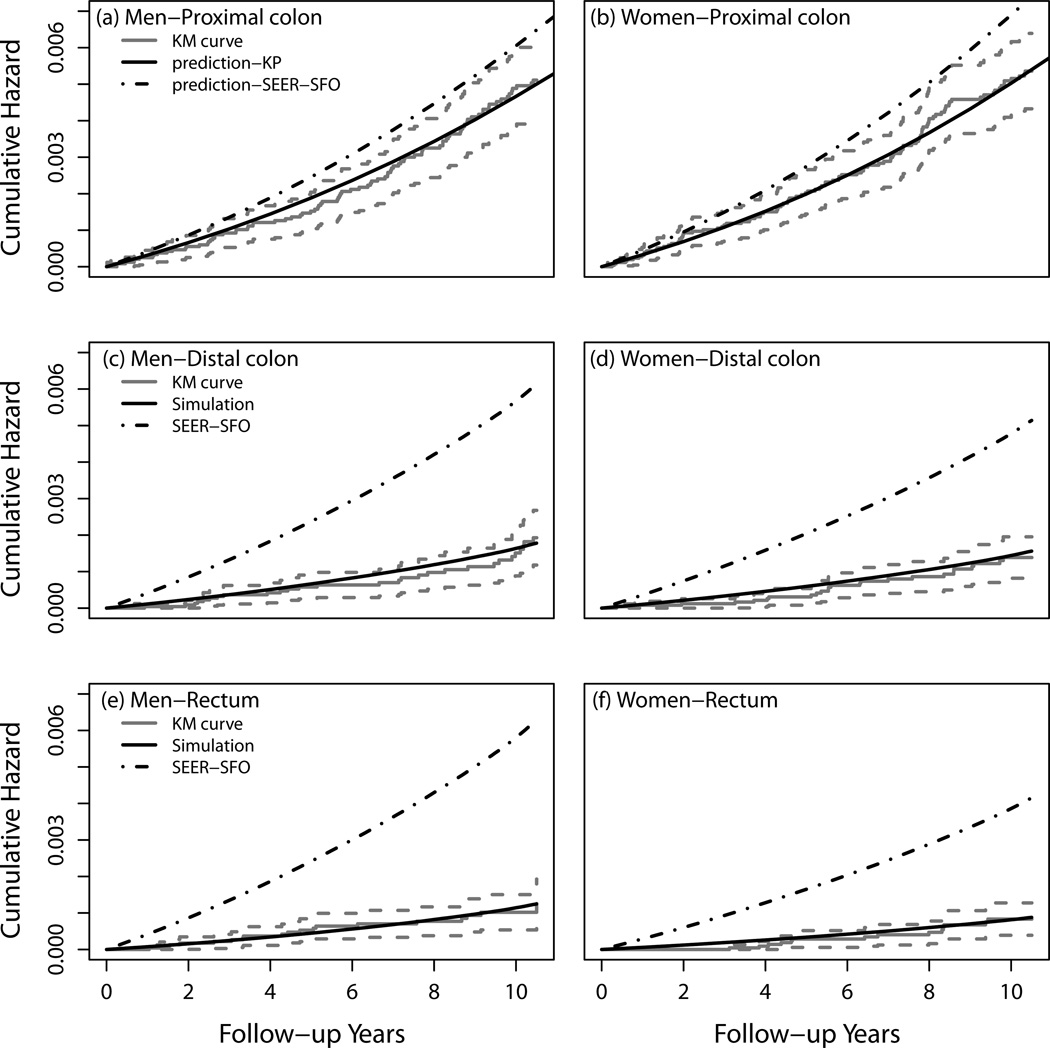
Methods: We calibrated models of CRC incidence within a multistage clonal expansion framework to data from: (1) San Francisco-Oakland SEER registry (reference population) and (2) FSG long-term follow-up data from 50,757 individuals after a negative FSG in the Kaiser Permanente system. We compared the residual CRC risks after FSG with full-length colonoscopy.
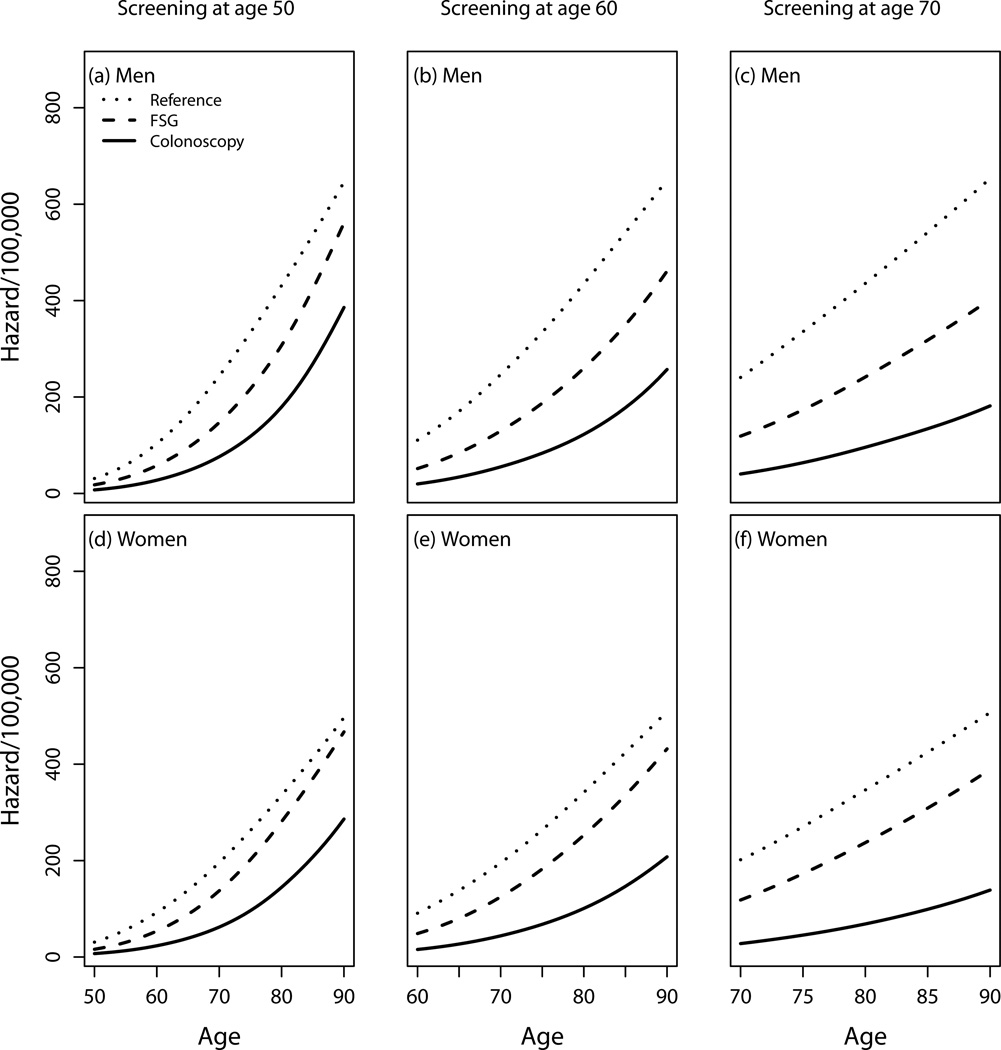
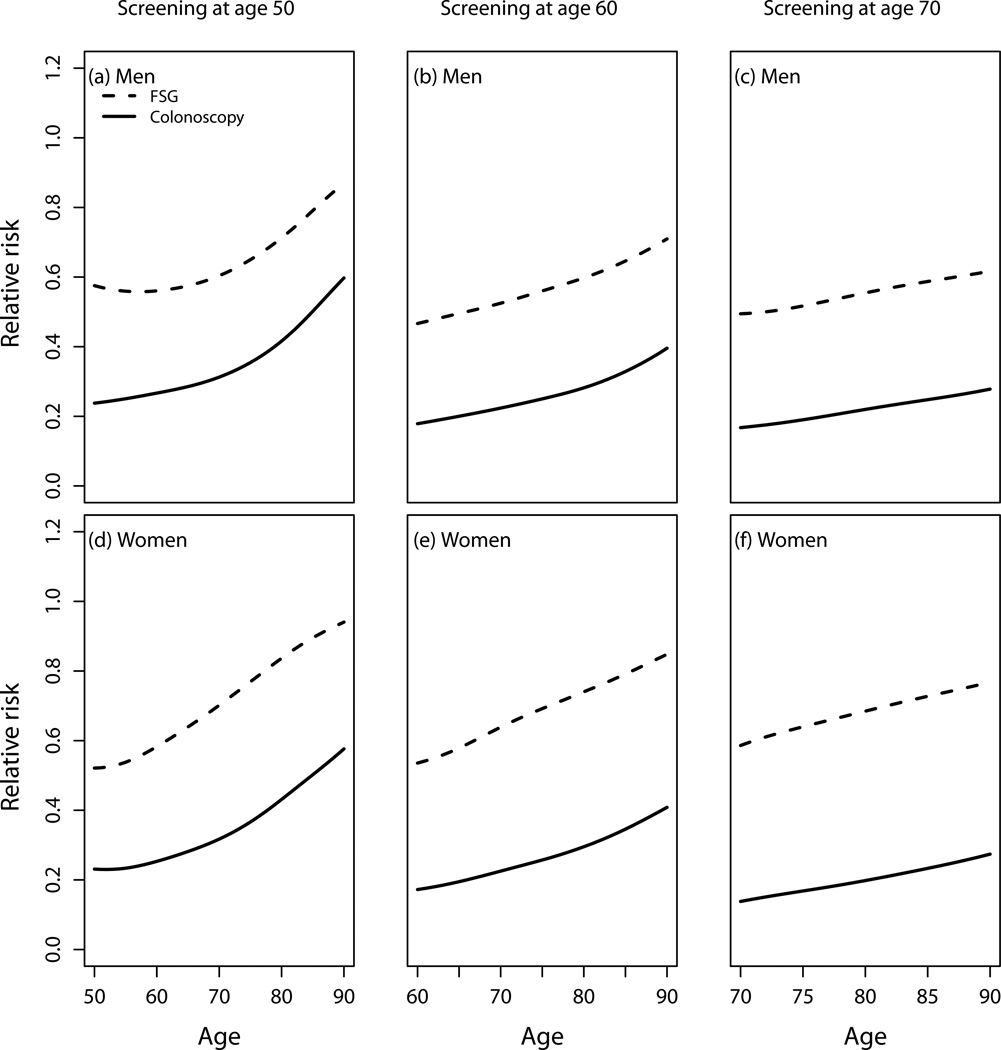
Results: Our model mirrors trial data with 10-year CRC risk reductions after FSG screening at age 50 years of approximately one-third; the optimal age for a 'once-only' FSG exam was between ages 50 and 60 years; and the greater benefit was for men compared with women. There were considerable incremental gains in reduction in CRC risk by colonoscopy compared with FSG with the greatest benefit for screening colonoscopy at age 50 years. These results held up against lowering the right-sided adenoma detection sensitivity by 30%, as well as reducing the curative efficacy of polypectomy throughout the colon.
Conclusions: Mathematical modeling of CRC screening, which takes account of important aspects of tumor biology, demonstrates superior risk reductions by colonoscopy over FSG. Our predictions provide further rationale for recommending screening colonoscopy in average-risk populations before the age of 60.
Conflict of interest statement
Figures
Similar articles
-
Association of Colonoscopy Adenoma Findings With Long-term Colorectal Cancer Incidence.JAMA. 2018 May 15;319(19):2021-2031. doi: 10.1001/jama.2018.5809. JAMA. 2018. PMID: 29800214 Free PMC article. Clinical Trial.
-
How long does it take until the effects of endoscopic screening on colorectal cancer mortality are fully disclosed?: a Markov model study.Int J Cancer. 2018 Dec 1;143(11):2718-2724. doi: 10.1002/ijc.31716. Epub 2018 Sep 29. Int J Cancer. 2018. PMID: 29978478
-
Health benefits and cost-effectiveness of a hybrid screening strategy for colorectal cancer.Clin Gastroenterol Hepatol. 2013 Sep;11(9):1158-66. doi: 10.1016/j.cgh.2013.03.013. Epub 2013 Mar 28. Clin Gastroenterol Hepatol. 2013. PMID: 23542330
-
Options for screening for colorectal cancer.Scand J Gastroenterol Suppl. 2003;(237):13-6. doi: 10.1080/00855910310001421. Scand J Gastroenterol Suppl. 2003. PMID: 12797674 Review.
-
[Screening for colorectal cancer by endoscopy: rectosigmoidoscopy or coloscopy?].Rev Med Brux. 2001 Sep;22(4):A210-3. Rev Med Brux. 2001. PMID: 11680175 Review. French.
Cited by
-
African colorectal cancer burden in 2022 and projections to 2050.Ecancermedicalscience. 2024 Sep 26;18:1780. doi: 10.3332/ecancer.2024.1780. eCollection 2024. Ecancermedicalscience. 2024. PMID: 39430071 Free PMC article.
-
Early Life Exposures and Adult Cancer Risk.Epidemiol Rev. 2017 Jan 1;39(1):11-27. doi: 10.1093/epirev/mxx004. Epidemiol Rev. 2017. PMID: 28407101 Free PMC article. Review.
-
Determining Risk of Colorectal Cancer and Starting Age of Screening Based on Lifestyle, Environmental, and Genetic Factors.Gastroenterology. 2018 Jun;154(8):2152-2164.e19. doi: 10.1053/j.gastro.2018.02.021. Epub 2018 Feb 17. Gastroenterology. 2018. PMID: 29458155 Free PMC article.
-
Predicting colorectal cancer risk from adenoma detection via a two-type branching process model.PLoS Comput Biol. 2020 Feb 5;16(2):e1007552. doi: 10.1371/journal.pcbi.1007552. eCollection 2020 Feb. PLoS Comput Biol. 2020. PMID: 32023238 Free PMC article.
-
Effectiveness of Colonoscopy Screening vs Sigmoidoscopy Screening in Colorectal Cancer.JAMA Netw Open. 2024 Feb 5;7(2):e240007. doi: 10.1001/jamanetworkopen.2024.0007. JAMA Netw Open. 2024. PMID: 38421651 Free PMC article. Clinical Trial.
References
-
- Siegel RL, Ward EM, Jemal A. Trends in colorectal cancer incidence rates in the United States by tumor location and stage, 1992–2008. Cancer Epidemiol Biomarkers Prev. 2012;21(3):411–416. - PubMed
-
- Arnold M, Karim-Kos HE, Coebergh JW, Byrnes G, Antilla A, Ferlay J, Renehan AG, Forman D, Soerjomataram I. Recent trends in incidence of five common cancers in 26 European countries since 1988: Analysis of the European Cancer Registry database. Eur J Cancer. 2013 pii: S0959-8049(0913)00842-00843. - PubMed
-
- von Karsa L, Patnick J, Segnan N, Atkin W, Halloran S, Lansdorp-Vogelaar I, Malila N, Minozzi S, Moss S, Quirke P, Steele RJ, Vieth M, Aabakken L, Altenhofen L, Ancelle-Park R, Antoljak N, Anttila A, Armaroli P, Arrossi S, Austoker J, Banzi R, Bellisario C, Blom J, Brenner H, Bretthauer M, Camargo Cancela M, Costamagna G, Cuzick J, Dai M, Daniel J, Dekker E, Delicata N, Ducarroz S, Erfkamp H, Espinas JA, Faivre J, Faulds Wood L, Flugelman A, Frkovic-Grazio S, Geller B, Giordano L, Grazzini G, Green J, Hamashima C, Herrmann C, Hewitson P, Hoff G, Holten I, Jover R, Kaminski MF, Kuipers EJ, Kurtinaitis J, Lambert R, Launoy G, Lee W, Leicester R, Leja M, Lieberman D, Lignini T, Lucas E, Lynge E, Madai S, Marinho J, Maucec Zakotnik J, Minoli G, Monk C, Morais A, Muwonge R, Nadel M, Neamtiu L, Peris Tuser M, Pignone M, Pox C, Primic-Zakelj M, Psaila J, Rabeneck L, Ransohoff D, Rasmussen M, Regula J, Ren J, Rennert G, Rey J, Riddell RH, Risio M, Rodrigues V, Saito H, Sauvaget C, Scharpantgen A, Schmiegel W, Senore C, Siddiqi M, Sighoko D, Smith R, Smith S, Suchanek S, Suonio E, Tong W, Tornberg S, Van Cutsem E, Vignatelli L, Villain P, Voti L, Watanabe H, Watson J, Winawer S, Young G, Zaksas V, Zappa M, Valori R. European guidelines for quality assurance in colorectal cancer screening and diagnosis: overview and introduction to the full supplement publication. Endoscopy. 2013;45(1):51–59. - PMC - PubMed
-
- Atkin WS, Edwards R, Kralj-Hans I, Wooldrage K, Hart AR, Northover JM, Parkin DM, Wardle J, Duffy SW, Cuzick J Investigators UKFST. Once-only flexible sigmoidoscopy screening in prevention of colorectal cancer: a multicentre randomised controlled trial. Lancet. 2010;375(9726):1624–1633. - PubMed
-
- Segnan N, Armaroli P, Bonelli L, Risio M, Sciallero S, Zappa M, Andreoni B, Arrigoni A, Bisanti L, Casella C, Crosta C, Falcini F, Ferrero F, Giacomin A, Giuliani O, Santarelli A, Visioli CB, Zanetti R, Atkin WS, Senore C, Group SW. Once-only sigmoidoscopy in colorectal cancer screening: follow-up findings of the Italian Randomized Controlled Trial--SCORE. Journal of the National Cancer Institute. 2011;103(17):1310–1322. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
