

Body composition and bone mineral density after ovarian hormone suppression with or without estradiol treatment
- PMID: 25783468
- PMCID: PMC4760356
- DOI: 10.1097/GME.0000000000000430
Body composition and bone mineral density after ovarian hormone suppression with or without estradiol treatment
Erratum in
-
Body composition and bone mineral density after ovarian hormone suppression with or without estradiol treatment: Erratum.Menopause. 2018 Mar;25(3):359. doi: 10.1097/GME.0000000000001056. Menopause. 2018. PMID: 29465503 No abstract available.
Abstract
Objective: Suppression of ovarian hormones in premenopausal women on gonadotropin-releasing hormone agonist (GnRH(AG)) therapy can cause fat mass (FM) gain and fat-free mass (FFM) loss. Whether this is specifically caused by a decline in serum estradiol (E2) is unknown. This study aims to evaluate the effects of GnRH(AG) with placebo (PL) or E2 add-back therapy on FM, FFM, and bone mineral density (BMD). Our exploratory aim was to evaluate the effects of resistance exercise training on body composition during the drug intervention.
Methods: Seventy healthy premenopausal women underwent 5 months of GnRH(AG) therapy and were randomized to receive transdermal E2 (GnRH(AG) + E2, n = 35) or PL (GnRH(AG) + PL, n = 35) add-back therapy. As part of our exploratory aim to evaluate whether exercise can minimize the effects of hormone suppression, some women within each drug arm were randomized to undergo a resistance exercise program (GnRH(AG) + E2 + Ex, n = 12; GnRH(AG) + PL + Ex, n = 12).
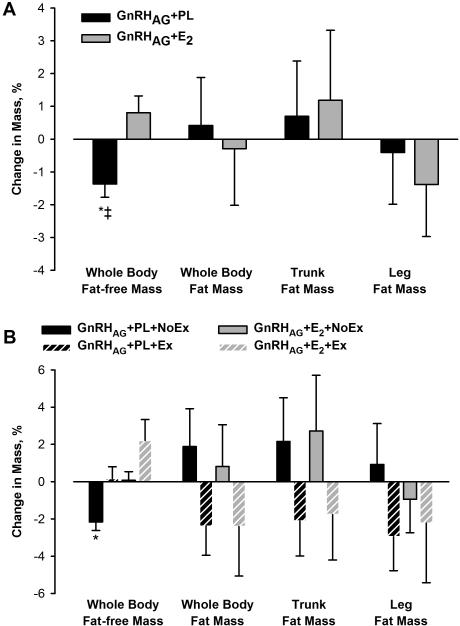
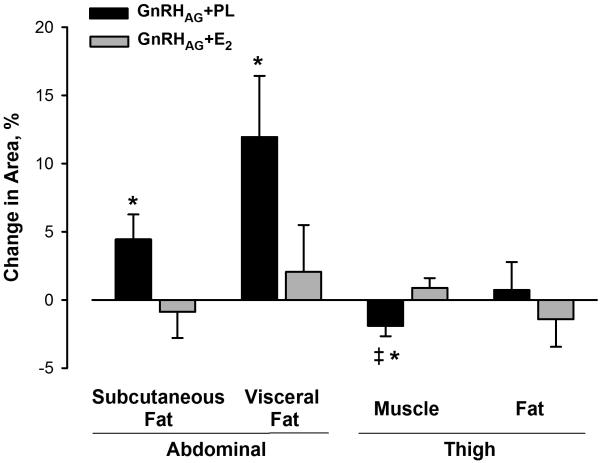
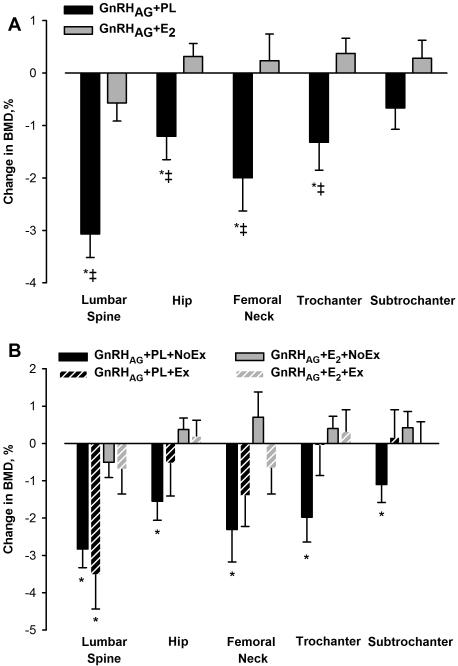
Results: The groups did not differ in mean (SD) age (36 [8] and 35 [9] y) or mean (SD) body mass index (both 28 [6] kg/m). FFM declined in response to GnRH(AG) + PL (mean, -0.6 kg; 95% CI, -1.0 to -0.3) but not in response to GnRH(AG) + E2 (mean, 0.3 kg; 95% CI, -0.2 to 0.8) or GnRH(AG) + PL + Ex (mean, 0.1 kg; 95% CI, -0.6 to 0.7). Although FM did not change in either group, visceral fat area increased in response to GnRH(AG) + PL but not in response to GnRH(AG) + E2. GnRH(AG) + PL induced a decrease in BMD at the lumbar spine and proximal femur that was prevented by E2. Preliminary data suggest that exercise may have favorable effects on FM, FFM, and hip BMD.
Conclusions: Suppression of ovarian E2 results in loss of bone and FFM and expansion of abdominal adipose depots. Failure of hormone suppression to increase total FM conflicts with previous studies of the effects of GnRH(AG). Further research is necessary to understand the role of estrogen in energy balance regulation and fat distribution.
Figures
Comment in
-
Visceral fat accumulation: is it caused by estrogen deficiency?Menopause. 2015 Oct;22(10):1030-1. doi: 10.1097/GME.0000000000000538. Menopause. 2015. PMID: 26397144 No abstract available.
Similar articles
-
Regulation of energy expenditure by estradiol in premenopausal women.J Appl Physiol (1985). 2015 Nov 1;119(9):975-81. doi: 10.1152/japplphysiol.00473.2015. Epub 2015 Sep 3. J Appl Physiol (1985). 2015. PMID: 26338457 Free PMC article. Clinical Trial.
-
Gonadotropin-releasing hormone agonist in premenopausal women does not alter hypothalamic-pituitary-adrenal axis response to corticotropin-releasing hormone.Am J Physiol Endocrinol Metab. 2018 Aug 1;315(2):E316-E325. doi: 10.1152/ajpendo.00221.2017. Epub 2018 Apr 6. Am J Physiol Endocrinol Metab. 2018. PMID: 29631362 Free PMC article. Clinical Trial.
-
Hormonal Add-Back Therapy for Females Treated With Gonadotropin-Releasing Hormone Agonist for Endometriosis: A Randomized Controlled Trial.Obstet Gynecol. 2015 Sep;126(3):617-627. doi: 10.1097/AOG.0000000000000964. Obstet Gynecol. 2015. PMID: 26181088 Free PMC article. Clinical Trial.
-
Add-back therapy and gonadotropin-releasing hormone agonists in the treatment of patients with endometriosis: can a consensus be reached? Add-Back Consensus Working Group.Fertil Steril. 1999 Mar;71(3):420-4. doi: 10.1016/s0015-0282(98)00500-7. Fertil Steril. 1999. PMID: 10065775 Review.
-
Clinical efficacy of add-back therapy in treatment of endometriosis: a meta-analysis.Arch Gynecol Obstet. 2014 Sep;290(3):513-23. doi: 10.1007/s00404-014-3230-8. Epub 2014 Apr 13. Arch Gynecol Obstet. 2014. PMID: 24728145 Review.
Cited by
-
Dietary Intake and Energy Expenditure in Breast Cancer Survivors: A Review.Nutrients. 2021 Sep 27;13(10):3394. doi: 10.3390/nu13103394. Nutrients. 2021. PMID: 34684403 Free PMC article. Review.
-
Modeling Diet-Induced Obesity with Obesity-Prone Rats: Implications for Studies in Females.Front Nutr. 2016 Nov 24;3:50. doi: 10.3389/fnut.2016.00050. eCollection 2016. Front Nutr. 2016. PMID: 27933296 Free PMC article. Review.
-
Regulation of energy expenditure by estradiol in premenopausal women.J Appl Physiol (1985). 2015 Nov 1;119(9):975-81. doi: 10.1152/japplphysiol.00473.2015. Epub 2015 Sep 3. J Appl Physiol (1985). 2015. PMID: 26338457 Free PMC article. Clinical Trial.
-
Brown Adipose Tissue-A Translational Perspective.Endocr Rev. 2023 Mar 4;44(2):143-192. doi: 10.1210/endrev/bnac015. Endocr Rev. 2023. PMID: 35640259 Free PMC article. Review.
-
Modulation of Energy Expenditure by Estrogens and Exercise in Women.Exerc Sport Sci Rev. 2018 Oct;46(4):232-239. doi: 10.1249/JES.0000000000000160. Exerc Sport Sci Rev. 2018. PMID: 30001272 Free PMC article. Review.
References
-
- Stein CJ, Colditz GA. The epidemic of obesity. J. Clin. Endocrinol. Metab. 2004 Jun;89(6):2522–2525. - PubMed
-
- Douchi T, Kuwahata R, Yamasaki H, et al. Inverse relationship between the changes in trunk lean and fat mass during gonadotropin-releasing hormone agonist therapy. Maturitas. 2002 May 20;42(1):31–35. - PubMed
-
- Douchi T, Kuwahata T, Yoshimitsu N, Iwamoto I, Yamasaki H, Nagata Y. Changes in serum leptin levels during GnRH agonist therapy. Endocr. J. 2003 Jun;50(3):355–359. - PubMed
-
- Dumesic DA, Abbott DH, Eisner JR, et al. Pituitary desensitization to gonadotropin-releasing hormone increases abdominal adiposity in hyperandrogenic anovulatory women. Fertil. Steril. 1998 Jul;70(1):94–101. - PubMed
-
- Revilla R, Revilla M, Villa LF, Cortes J, Arribas I, Rico H. Changes in body composition in women treated with gonadotropin-releasing hormone agonists. Maturitas. 1998 Nov 30;31(1):63–68. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
