

The Inferior Whorl For Detecting Diabetic Peripheral Neuropathy Using Corneal Confocal Microscopy
- PMID: 25783609
- PMCID: PMC4408884
- DOI: 10.1167/iovs.14-15919
The Inferior Whorl For Detecting Diabetic Peripheral Neuropathy Using Corneal Confocal Microscopy
Abstract
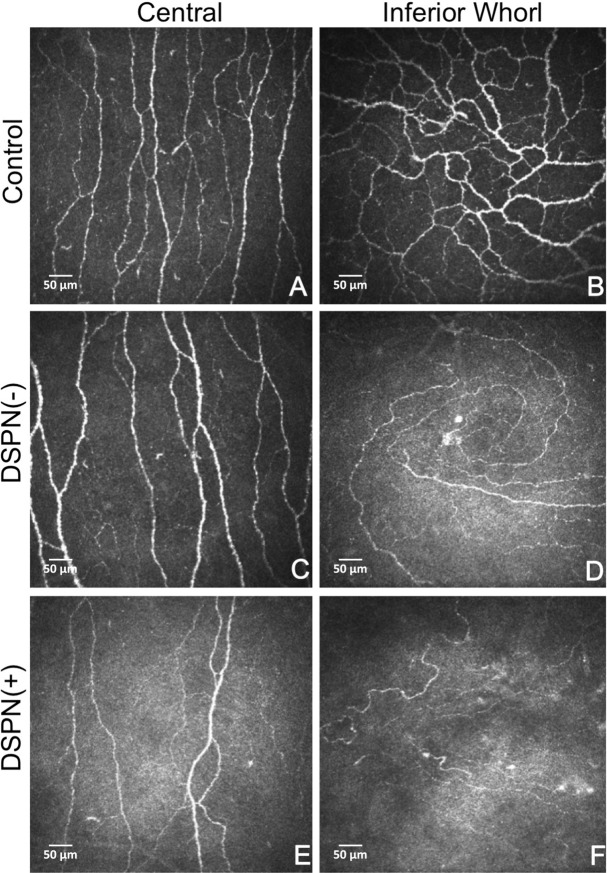
Purpose: In vivo corneal confocal microscopy (CCM) is increasingly used as a surrogate endpoint in studies of diabetic polyneuropathy (DPN). However, it is not clear whether imaging the central cornea provides optimal diagnostic utility for DPN. Therefore, we compared nerve morphology in the central cornea and the inferior whorl, a more distal and densely innervated area located inferior and nasal to the central cornea.
Methods: A total of 53 subjects with type 1/type 2 diabetes and 15 age-matched control subjects underwent detailed assessment of neuropathic symptoms (NPS), deficits (neuropathy disability score [NDS]), quantitative sensory testing (vibration perception threshold [VPT], cold and warm threshold [CT/WT], and cold- and heat-induced pain [CIP/HIP]), and electrophysiology (sural and peroneal nerve conduction velocity [SSNCV/PMNCV], and sural and peroneal nerve amplitude [SSNA/PMNA]) to diagnose patients with (DPN+) and without (DPN-) neuropathy. Corneal nerve fiber density (CNFD) and length (CNFL) in the central cornea, and inferior whorl length (IWL) were quantified.
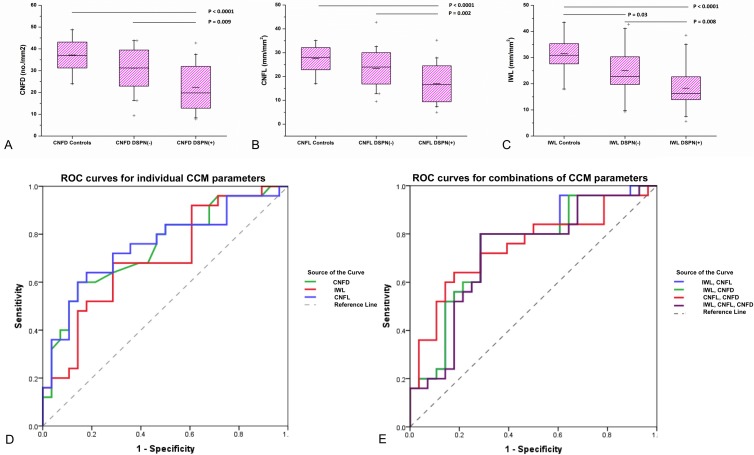
Results: Comparing control subjects to DPN- and DPN+ patients, there was a significant increase in NDS (0 vs. 2.6 ± 2.3 vs. 3.3 ± 2.7, P < 0.01), VPT (V; 5.4 ± 3.0 vs. 10.6 ± 10.3 vs. 17.7 ± 11.8, P < 0.01), WT (°C; 37.7 ± 3.5 vs. 39.1 ± 5.1 vs. 41.7 ± 4.7, P < 0.05), and a significant decrease in SSNCV (m/s; 50.2 ± 5.4 vs. 48.4 ± 5.0 vs. 39.5 ± 10.6, P < 0.05), CNFD (fibers/mm2; 37.8 ± 4.9 vs. 29.7 ± 7.7 vs. 27.1 ± 9.9, P < 0.01), CNFL (mm/mm2; 27.5 ± 3.6 vs. 24.4 ± 7.8 vs. 20.7 ± 7.1, P < 0.01), and IWL (mm/mm2; 35.1 ± 6.5 vs. 26.2 ± 10.5 vs. 23.6 ± 11.4, P < 0.05). For the diagnosis of DPN, CNFD, CNFL, and IWL achieved an area under the curve (AUC) of 0.75, 0.74, and 0.70, respectively, and a combination of IWL-CNFD achieved an AUC of 0.76.
Conclusions: The parameters of CNFD, CNFL, and IWL have a comparable ability to diagnose patients with DPN. However, IWL detects an abnormality even in patients without DPN. Combining IWL with CNFD may improve the diagnostic performance of CCM.
Figures
Similar articles
-
Diabetic Neuropathy Is Characterized by Progressive Corneal Nerve Fiber Loss in the Central and Inferior Whorl Regions.Invest Ophthalmol Vis Sci. 2020 Mar 9;61(3):48. doi: 10.1167/iovs.61.3.48. Invest Ophthalmol Vis Sci. 2020. PMID: 32232351 Free PMC article.
-
Greater corneal nerve loss at the inferior whorl is related to the presence of diabetic neuropathy and painful diabetic neuropathy.Sci Rep. 2018 Feb 19;8(1):3283. doi: 10.1038/s41598-018-21643-z. Sci Rep. 2018. PMID: 29459766 Free PMC article.
-
Corneal confocal microscopy for the diagnosis of diabetic peripheral neuropathy: A systematic review and meta-analysis.J Diabetes Investig. 2022 Jan;13(1):134-147. doi: 10.1111/jdi.13643. Epub 2021 Aug 27. J Diabetes Investig. 2022. PMID: 34351711 Free PMC article.
-
Corneal confocal microscopy compared with quantitative sensory testing and nerve conduction for diagnosing and stratifying the severity of diabetic peripheral neuropathy.BMJ Open Diabetes Res Care. 2020 Dec;8(2):e001801. doi: 10.1136/bmjdrc-2020-001801. BMJ Open Diabetes Res Care. 2020. PMID: 33355206 Free PMC article.
-
Corneal confocal microscopy for assessment of diabetic peripheral neuropathy: a meta-analysis.Br J Ophthalmol. 2016 Jan;100(1):9-14. doi: 10.1136/bjophthalmol-2014-306038. Epub 2015 Feb 12. Br J Ophthalmol. 2016. PMID: 25677672 Review.
Cited by
-
Reproducibility of In Vivo Corneal Confocal Microscopy Using an Automated Analysis Program for Detection of Diabetic Sensorimotor Polyneuropathy.PLoS One. 2015 Nov 5;10(11):e0142309. doi: 10.1371/journal.pone.0142309. eCollection 2015. PLoS One. 2015. PMID: 26539984 Free PMC article.
-
The Utility of Corneal Nerve Fractal Dimension Analysis in Peripheral Neuropathies of Different Etiology.Transl Vis Sci Technol. 2020 Aug 28;9(9):43. doi: 10.1167/tvst.9.9.43. eCollection 2020 Aug. Transl Vis Sci Technol. 2020. PMID: 32934893 Free PMC article.
-
Using corneal confocal microscopy to compare Mecobalamin intramuscular injections vs oral tablets in treating diabetic peripheral neuropathy: a RCT.Sci Rep. 2021 Jul 19;11(1):14697. doi: 10.1038/s41598-021-94284-4. Sci Rep. 2021. PMID: 34282267 Free PMC article. Clinical Trial.
-
Diagnosis of Neuropathy and Risk Factors for Corneal Nerve Loss in Type 1 and Type 2 Diabetes: A Corneal Confocal Microscopy Study.Diabetes Care. 2021 Jan;44(1):150-156. doi: 10.2337/dc20-1482. Epub 2020 Nov 3. Diabetes Care. 2021. PMID: 33144353 Free PMC article.
-
Correlation Between Corneal Whorl-Like Nerve and Retinal Neurodegenerative Changes and Their Association With Microvessel Perfusion in Diabetes.Invest Ophthalmol Vis Sci. 2023 Nov 1;64(14):44. doi: 10.1167/iovs.64.14.44. Invest Ophthalmol Vis Sci. 2023. PMID: 38019489 Free PMC article.
References
-
- Dyck P,, Kratz K,, Karnes J,, et al. The prevalence by staged severity of various types of diabetic neuropathy, retinopathy, and nephropathy in a population based cohort: The Rochester Diabetic Neuropathy Study. Neurology. 1993; 43: 817–824. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
