

Pneumonia in the neutropenic cancer patient
- PMID: 25784246
- PMCID: PMC4429304
- DOI: 10.1097/MCP.0000000000000156
Pneumonia in the neutropenic cancer patient
Abstract
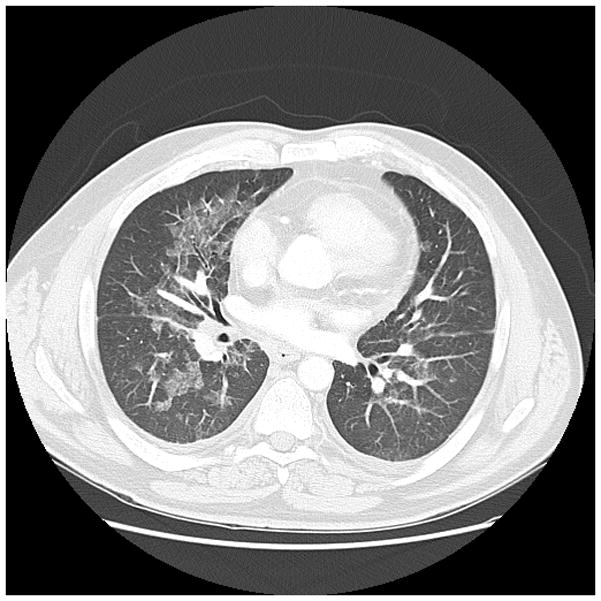
Purpose of review: Pneumonia is the leading cause of death among neutropenic cancer patients, particularly those with acute leukaemia. Even with empiric therapy, case fatality rates of neutropenic pneumonias remain unacceptably high. However, recent advances in the management of neutropenic pneumonia offer hope for improved outcomes in the cancer setting. This review summarizes recent literature regarding the clinical presentation, microbiologic trends, diagnostic advances and therapeutic recommendations for cancer-related neutropenic pneumonia.
Recent findings: Although neutropenic patients acquire pathogens both in community and nosocomial settings, patients' obligate healthcare exposures result in the frequent identification of multidrug-resistant bacterial organisms on conventional culture-based assessment of respiratory secretions. Modern molecular techniques, including expanded use of galactomannan testing, have further facilitated identification of fungal pathogens, allowing for aggressive interventions that appear to improve patient outcomes. Multiple interested societies have issued updated guidelines for antibiotic therapy of suspected neutropenic pneumonia. The benefit of antibiotic medications may be further enhanced by agents that promote host responses to infection.
Summary: Neutropenic cancer patients have numerous potential causes for pulmonary infiltrates and clinical deterioration, with lower respiratory tract infections among the most deadly. Early clinical suspicion, diagnosis and intervention for neutropenic pneumonia provide cancer patients' best hope for survival.
Conflict of interest statement
DEO has no financial conflicts of interest to disclose.
SEE is an author on US Patent 8,883,174 entitled “Compositions for stimulation of mammalian innate immune responses to pathogens,” and owns stock in Pulmotect, Inc., a company that has licensed technology referenced in this manuscript for clinical development.
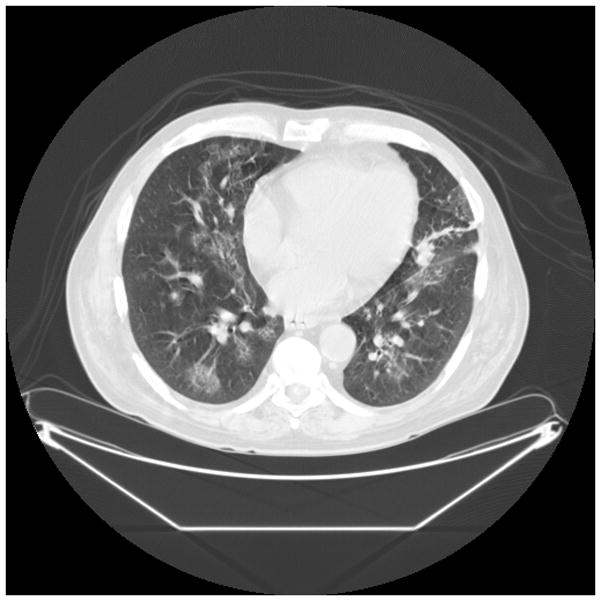
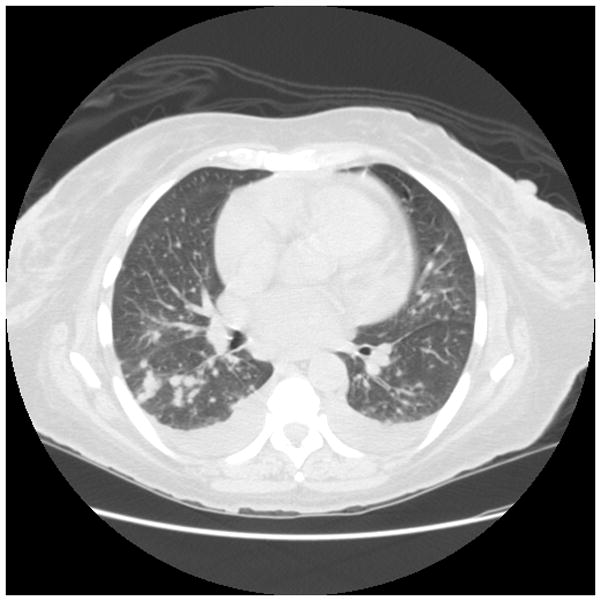
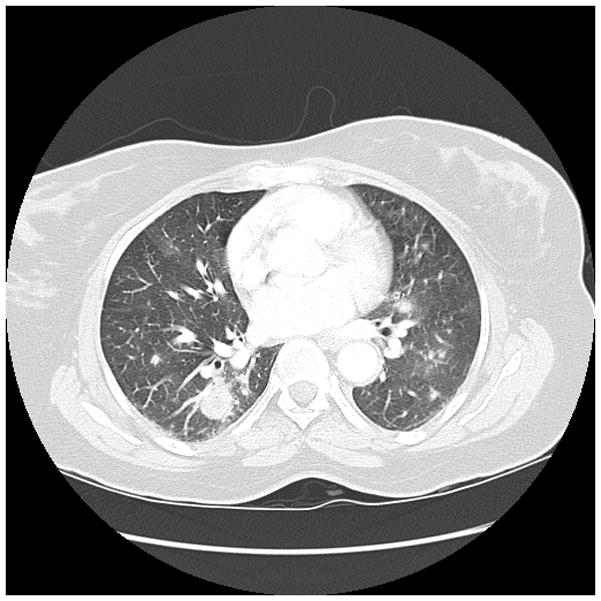
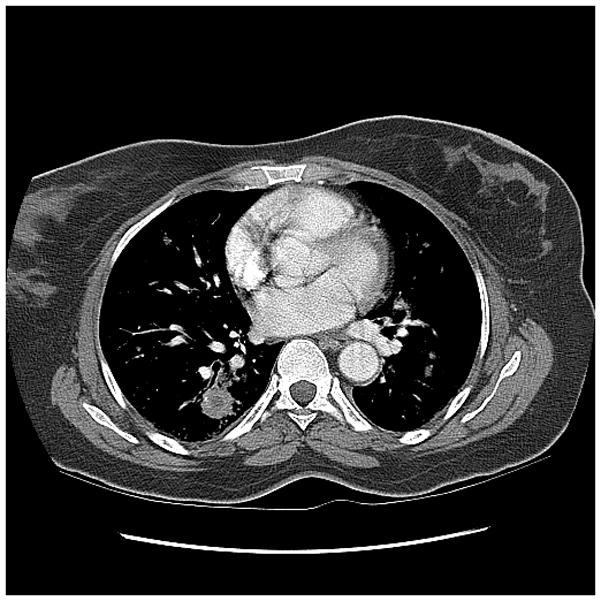
Figures

References
-
- Joos L, Tamm M. Breakdown of pulmonary host defense in the immunocompromised host: cancer chemotherapy. Proc Am Thorac Soc. 2005;2(5):445–8. - PubMed
-
- WHO. The World Health Report 2004 -- Changing History. Geneva: World Health Organization; 2004.
-
- Ahmed S, Siddiqui AK, Rossoff L, Sison CP, Rai KR. Pulmonary complications in chronic lymphocytic leukemia. Cancer. 2003;98(9):1912–7. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
