

Proposed management protocol for ingested esophageal foreign body and aortoesophageal fistula: a single-center experience
- PMID: 25785035
- PMCID: PMC4358490
Proposed management protocol for ingested esophageal foreign body and aortoesophageal fistula: a single-center experience
Abstract
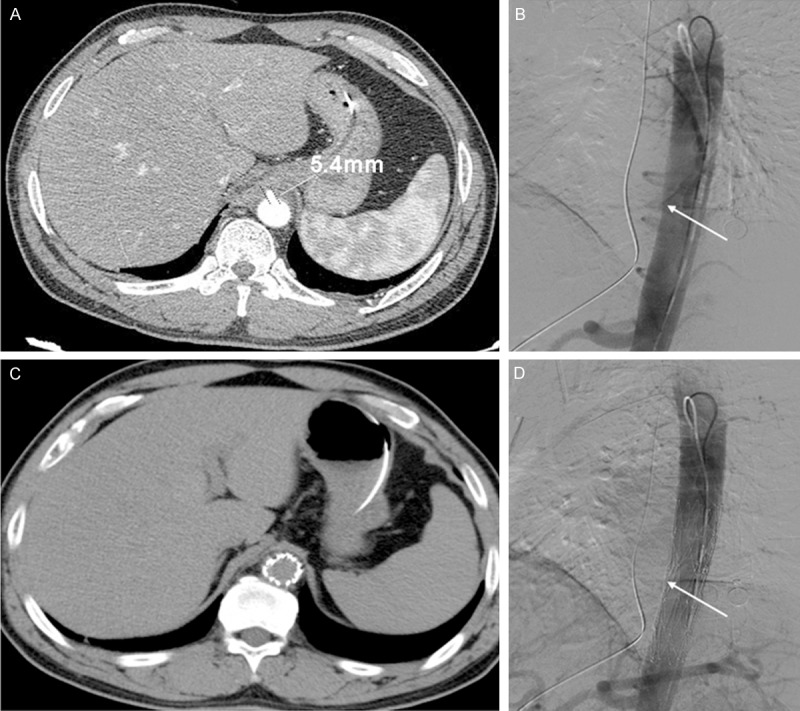
Objective: Aortoesophageal fistula (AEF) is a life-threatening complication of foreign body ingestion. The primary objective of this study was to describe a new management protocol for infected AEFs, which combines endovascular stent grafting and mediastinal drainage using video-assisted thoracoscopic surgery (VATS).
Methods: The authors analyzed the clinical data of 22 patients with ingested foreign bodies retrospectively, developed a classification system based on multidetector computed tomography (MDCT) findings for esophageal injuries induced by foreign body ingestion, and used this system and the clinical presentation to guide treatment.
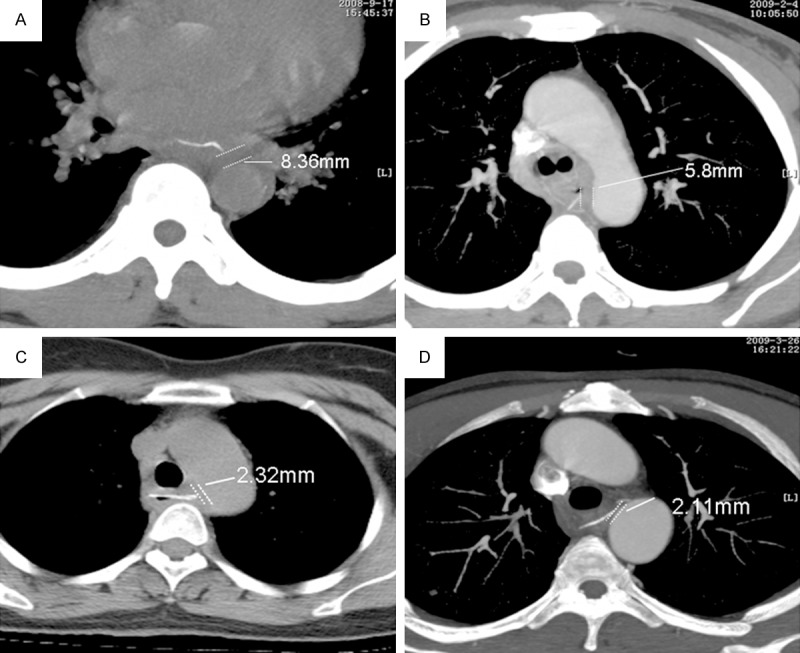
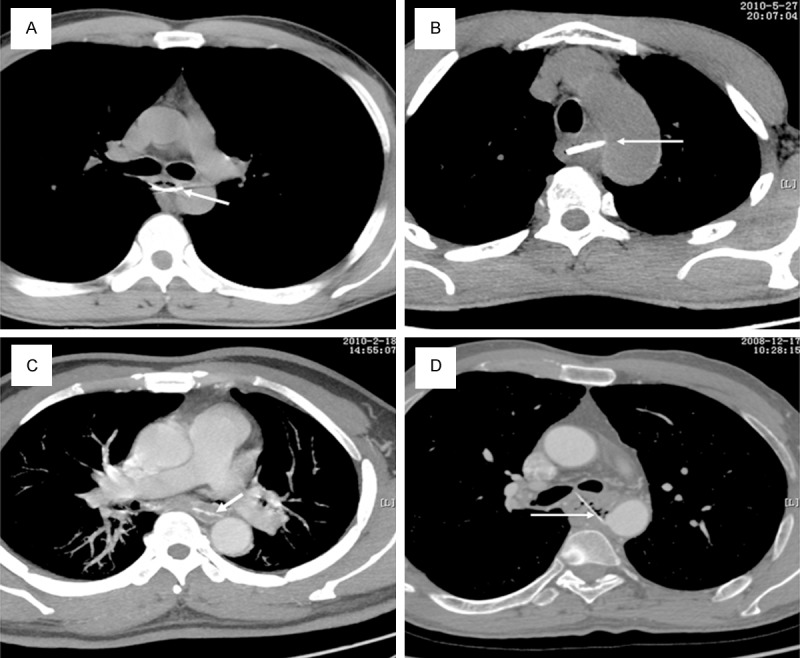
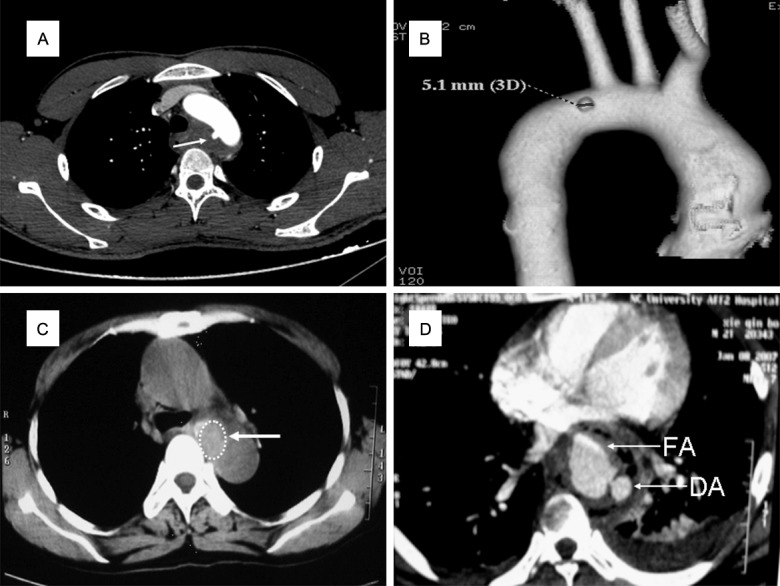
Results: Depending on the MDCT findings, the esophageal injuries were divided into four grades: Grade I, non-penetrating injury (six patients); Grade II, penetrating injury with minimal infection (five patients); Grade III, potential AEF (five patients); and Grade IV, definite AEF (six patients). When a foreign body was visible on MDCT, a distance of ≤ 2 mm between the foreign body and aortic wall indicated potential or definite AEF. When no foreign body was visible, a typical clinical presentation, especially sentinel hemorrhage, and MDCT findings were used to establish the diagnosis. Only three Grade IV patients who underwent open surgery died of severe hemorrhage within 24 h postoperatively. The others patients had a good outcome with different treatment.
Conclusions: The authors' experience indicates that MDCT was useful to classify esophageal injuries caused by foreign body ingestion which predicted the risk of AEF; endovascular stent grafting and VATS-guided mediastinal drainage would be a safe and minimally invasive method for treating patients with AEF and has the potential for improved treatment options for AEFs.
Keywords: Aortoesophageal fistula; endovascular stenting; esophageal foreign body; video-assisted thoracoscopic surgery.
Figures
References
-
- Gobolos L, Miskolczi S, Pousios D, Tsang GM, Livesey SA, Barlow CW, Kaarne M, Shambrook J, Lipnevicius A, Ohri SK. Management options for aorto-oesophageal fistula: case histories and review of the literature. Perfusion. 2013;28:286–290. - PubMed
-
- Chiari H. Uber Pemdkorperve rletzung des Oesophagus mit Aorten-perforation. Berl Klin Wochenschr. 1914;51:7–9.
-
- Sager HB, Wellhoner P, Wermelt JA, Schunkert H, Kurowski V. Lethal Hemorrhage Caused by Aortoesophageal Fistula Secondary to Stent-Graft Repair of the Thoracic Aorta. Cardiovasc Intervent Radiol. 2011 [Epub ahead of print] - PubMed
-
- Venara A, Hamdi S, Desolneux G, Papon X, Lermite E, Arnaud JP. Long-term successful management of an aortoesophageal fistula secondary to the ingestion of a bone. Presse Med. 2012;41:543–546. - PubMed
-
- Ctercteko G, Mok CK. Aorta-esophageal fistula induced by a foreign body: the first recorded survival. J Thorac Cardiovasc Surg. 1980;80:233–235. - PubMed
LinkOut - more resources
Full Text Sources