

Peritoneal carcinomatosis: intraoperative parameters in open (coliseum) versus closed abdomen HIPEC
- PMID: 25785194
- PMCID: PMC4345051
- DOI: 10.1155/2015/610597
Peritoneal carcinomatosis: intraoperative parameters in open (coliseum) versus closed abdomen HIPEC
Abstract
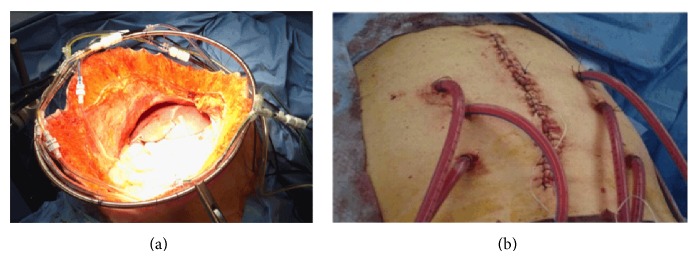
Background: Peritoneal carcinomatosis (PC) is associated with a poor prognosis. Cytoreductive surgery (CRS) and HIPEC play an important role in well-selected patients with PC. The aim of the study is to present the differences in the intraoperative parameters in patients who received HIPEC in two different manners, open versus closed abdomen.
Patients and methods: The population includes 105 patients with peritoneal carcinomatosis from colorectal, gastric, and ovarian cancer, sarcoma, mesothelioma, and pseudomyxoma peritonei. Group A (n = 60) received HIPEC using the open technique and Group B (n = 45) received HIPEC with the closed technique. The main end points were morbidity, mortality, and overall hospital stay.
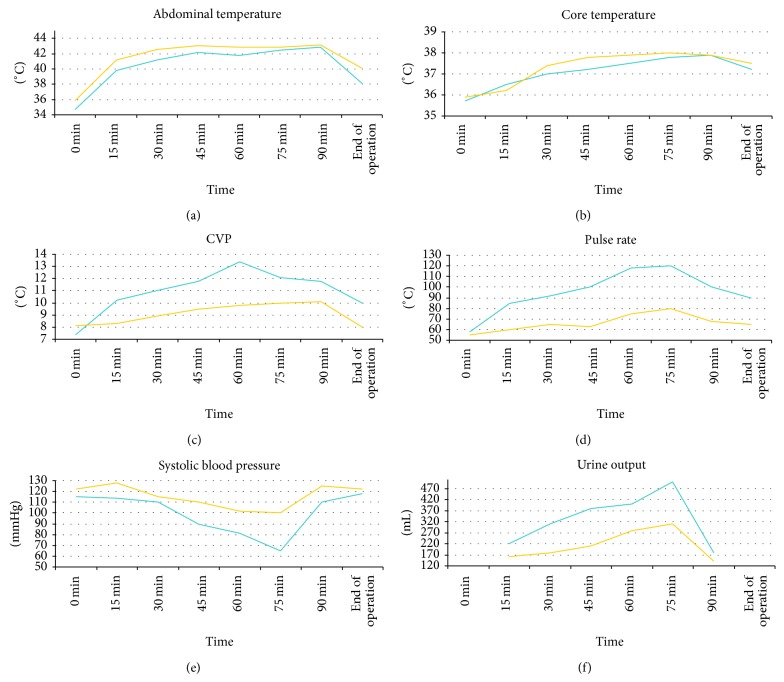
Results: There were two postoperative deaths (3.3%) in the open group versus no deaths in the closed group. Twenty-two patients in the open group (55%) had grade III-IV complications versus 18 patients in the closed group (40%). There are more stable intraoperative conditions in the closed abdomen HIPEC in CVP, pulse rate, and systolic pressure parameters.
Conclusions: Both methods are equal in the HIPEC procedures. Perhaps the closed method is the method of choice for frail patients due to more stable hemodynamic parameters.
Figures
References
-
- Pascual-Ramírez J., Sánchez García S., González Ruiz de la Herrán F., et al. Security and efficiency of a closed-system, turbulent-flow circuit for hyperthermic intraperitoneal chemotherapy after cytoreductive ovarian surgery: perioperative outputs. Archives of Gynecology and Obstetrics. 2014;290(1):121–129. doi: 10.1007/s00404-014-3153-4. - DOI - PubMed
-
- Rankovic V. I., Masirevic V. P., Pavlov M. J., et al. Hemodynamic and cardiovascular problems during modified hyperthermic intraperitoneal perioperative chemotherapy. Hepato-Gastroenterology. 2007;54(74):364–366. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
