

Outcome of concurrent occult hemothorax and pneumothorax in trauma patients who required assisted ventilation
- PMID: 25785199
- PMCID: PMC4345256
- DOI: 10.1155/2015/859130
Outcome of concurrent occult hemothorax and pneumothorax in trauma patients who required assisted ventilation
Abstract
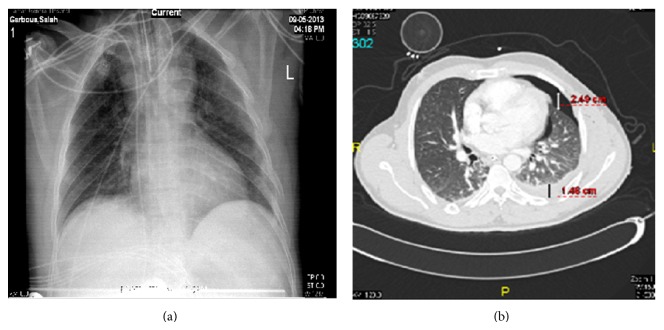
Background. The management and outcomes of occult hemopneumothorax in blunt trauma patients who required mechanical ventilation are not well studied. We aimed to study patients with occult hemopneumothorax on mechanical ventilation who could be carefully managed without tube thoracostomy. Methods. Chest trauma patients with occult hemopneumothorax who were on mechanical ventilation were prospectively evaluated. The presence of hemopneumothorax was confirmed by CT scanning. Hospital length of stay, complications, and outcome were recorded. Results. A total of 56 chest trauma patients with occult hemopneumothorax who were on ventilatory support were included with a mean age of 36 ± 13 years. Hemopneumothorax was managed conservatively in 72% cases and 28% underwent tube thoracostomy as indicated. 29% of patients developed pneumonia, 16% had Acute Respiratory Distress Syndrome (ARDS), and 7% died. Thickness of hemothorax, duration of mechanical ventilation, and development of ARDS were significantly associated with tube thoracostomy in comparison to no-chest tube group. Conclusions. The majority of occult hemopneumothorax can be carefully managed without tube thoracostomy in patients who required positive pressure ventilation. Tube thoracotomy could be restricted to those who had evidence of increase in the size of the hemothorax or pneumothorax on follow-up chest radiographs or developed respiratory compromise.
Figures



Similar articles
-
Occult Pneumothorax in Patients Presenting with Blunt Chest Trauma: An Observational Analysis.Qatar Med J. 2020 Mar 16;2020(1):10. doi: 10.5339/qmj.2020.10. eCollection 2020. Qatar Med J. 2020. PMID: 32206592 Free PMC article.
-
Occult hemopneumothorax following chest trauma does not need a chest tube.Eur J Trauma Emerg Surg. 2013 Feb;39(1):43-6. doi: 10.1007/s00068-012-0210-1. Epub 2012 Jul 20. Eur J Trauma Emerg Surg. 2013. PMID: 26814922
-
Occult pneumothorax in blunt trauma: is there a need for tube thoracostomy?Eur J Trauma Emerg Surg. 2016 Dec;42(6):785-790. doi: 10.1007/s00068-016-0645-x. Epub 2016 Feb 10. Eur J Trauma Emerg Surg. 2016. PMID: 26860113
-
The management of occult hemothorax in adults with thoracic trauma: A systematic review and meta-analysis.J Trauma Acute Care Surg. 2020 Dec;89(6):1225-1232. doi: 10.1097/TA.0000000000002936. J Trauma Acute Care Surg. 2020. PMID: 32925577
-
Pneumothorax in patients with respiratory failure in ICU.J Thorac Dis. 2021 Aug;13(8):5195-5204. doi: 10.21037/jtd-19-3752. J Thorac Dis. 2021. PMID: 34527359 Free PMC article. Review.
Cited by
-
Analysis of oxidative stress-related markers in critically ill polytrauma patients: An observational prospective single-center study.Bosn J Basic Med Sci. 2018 May 20;18(2):191-197. doi: 10.17305/bjbms.2018.2306. Bosn J Basic Med Sci. 2018. PMID: 29310566 Free PMC article.
-
TM9SF1 offers utility as an efficient predictor of clinical severity and mortality among acute respiratory distress syndrome patients.Front Immunol. 2024 Jun 3;15:1408406. doi: 10.3389/fimmu.2024.1408406. eCollection 2024. Front Immunol. 2024. PMID: 38887291 Free PMC article.
-
Intraoperative Tension Pneumothorax in a Patient With Remote Trauma and Previous Tracheostomy.J Investig Med High Impact Case Rep. 2016 Feb 29;4(1):2324709616636397. doi: 10.1177/2324709616636397. eCollection 2016 Jan-Mar. J Investig Med High Impact Case Rep. 2016. PMID: 27006957 Free PMC article.
-
Occult Pneumothorax in Patients Presenting with Blunt Chest Trauma: An Observational Analysis.Qatar Med J. 2020 Mar 16;2020(1):10. doi: 10.5339/qmj.2020.10. eCollection 2020. Qatar Med J. 2020. PMID: 32206592 Free PMC article.
-
Management of computed tomography-detected pneumothorax in patients with blunt trauma: experience from a community-based hospital.Singapore Med J. 2018 Mar;59(3):150-154. doi: 10.11622/smedj.2017074. Epub 2017 Jul 25. Singapore Med J. 2018. PMID: 28741012 Free PMC article.
References
-
- Livingston D. H., Hauser C. J. Trauma to the chest wall and lung. In: Moore E. E., Feliciano D. V., Mattox K. L., editors. Trauma. 5th. New York, NY, USA: McGraw-Hill; 1995. pp. 507–537.
LinkOut - more resources
Full Text Sources
Other Literature Sources
