

Host response to Candida albicans bloodstream infection and sepsis
- PMID: 25785541
- PMCID: PMC4601378
- DOI: 10.4161/21505594.2014.988096
Host response to Candida albicans bloodstream infection and sepsis
Abstract
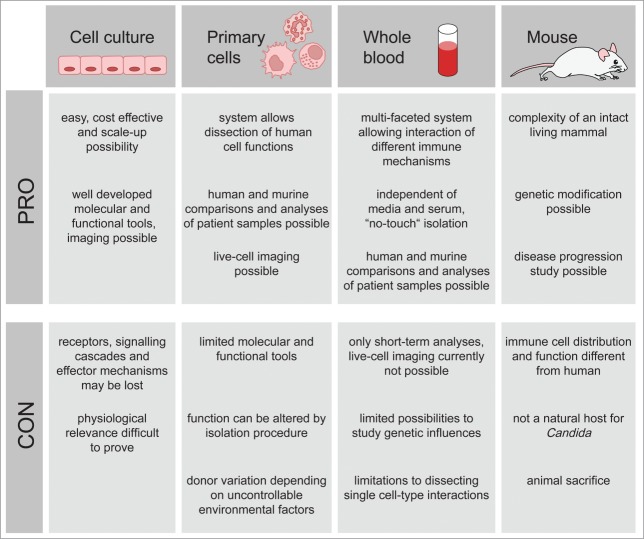
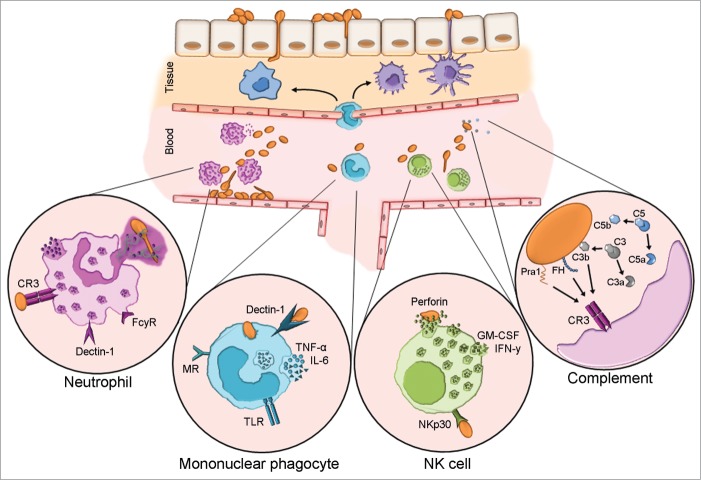
Candida albicans is a major cause of bloodstream infection which may present as sepsis and septic shock - major causes of morbidity and mortality world-wide. After invasion of the pathogen, innate mechanisms govern the early response. Here, we outline the models used to study these mechanisms and summarize our current understanding of innate immune responses during Candida bloodstream infection. This includes protective immunity as well as harmful responses resulting in Candida induced sepsis. Neutrophilic granulocytes are considered principal effector cells conferring protection and recognize C. albicans mainly via complement receptor 3. They possess a range of effector mechanisms, contributing to elimination of the pathogen. Neutrophil activation is closely linked to complement and modulated by activated mononuclear cells. A thorough understanding of these mechanisms will help in creating an individualized approach to patients suffering from systemic candidiasis and aid in optimizing clinical management.
Keywords: Candida albicans; bloodsteam infection; innate immune response; sepsis.
Figures
References
-
- Mayr FB, Yende S, Angus DC. Epidemiology of severe sepsis. Virulence 2014; 5:4-11; PMID:24335434; http://dx.doi.org/10.4161/viru.27372 - DOI - PMC - PubMed
-
- Martin GS, Mannino DM, Eaton S, Moss M. The epidemiology of sepsis in the United States from 1979 through 2000. N Engl J Med 2003; 348:1546-54; PMID:12700374; http://dx.doi.org/10.1056/NEJMoa022139 - DOI - PubMed
-
- Lionakis MS. New insights into innate immune control of systemic candidiasis. Med Mycol 2014; 52:555-64; PMID:25023483; http://dx.doi.org/10.1093/mmy/myu029 - DOI - PMC - PubMed
-
- Leleu C, Gloria E, Renault G, Barrey E. Analysis of trotter gait on the track by accelerometry and image analysis. Equine Vet J Suppl 2002:344-8; PMID:12405713 - PubMed
-
- Kollef M, Micek S, Hampton N, Doherty JA, Kumar A. Septic shock attributed to Candida infection: importance of empiric therapy and source control. Clin Infect Dis 2012; 54:1739-46; PMID:22423135; http://dx.doi.org/10.1093/cid/cis305 - DOI - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical