

Understanding stand-to-sit maneuver: implications for motor system neuroprostheses after paralysis
- PMID: 25786073
- PMCID: PMC4392895
- DOI: 10.1682/JRRD.2013.12.0264
Understanding stand-to-sit maneuver: implications for motor system neuroprostheses after paralysis
Abstract
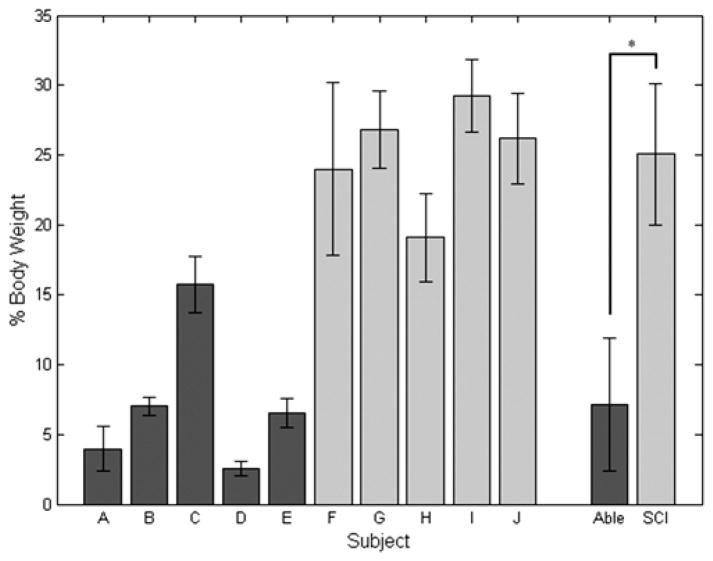
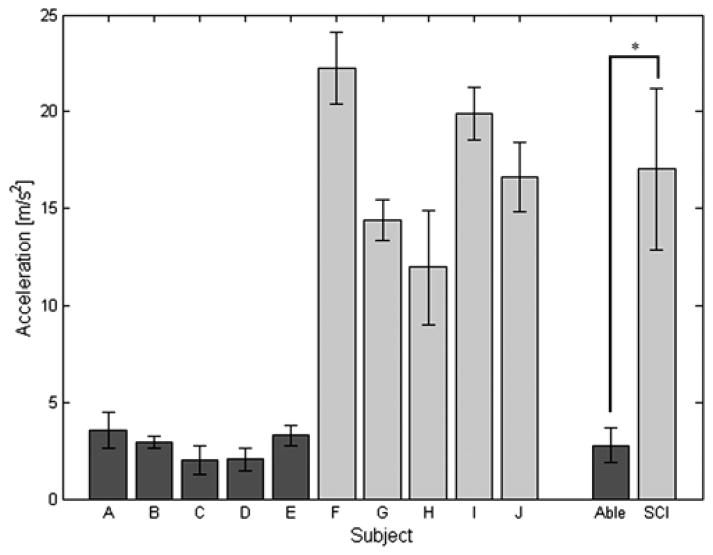
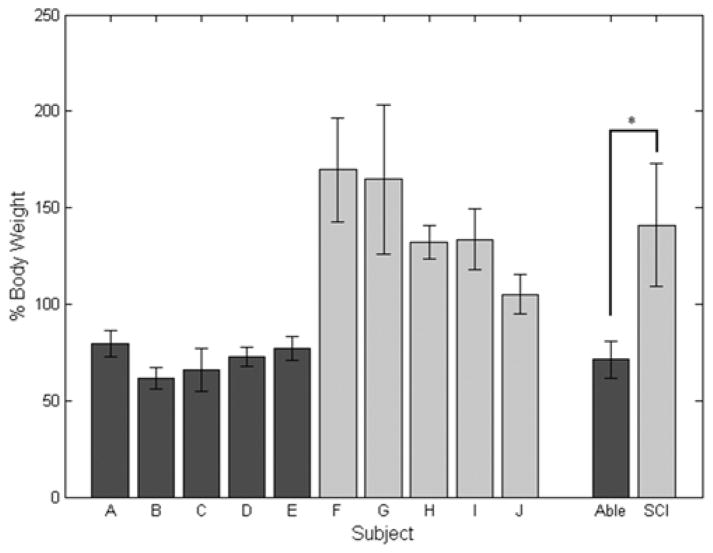
Standing up, standing, and walking functions can be restored to people with spinal cord injury by contracting the paralyzed hip, knee, and ankle muscles with electrical stimulation. Restoring these functions using electrical stimulation requires controlled activation to provide coordinated movements. However, the stand-to-sit (STS) maneuver involves eccentric contractions of the quadriceps to control lowering of the body to the seated position, which is difficult to achieve with stimulation alone and presents unique challenges to lower-limb neuroprostheses. In this study, we examined the biomechanics of the STS maneuver in five nondisabled individuals and five users of an implanted neuroprosthesis. Neuroprosthesis users relied heavily on their upper limbs during STS, with peak supporting forces approximately 25% body weight, and exhibited an average vertical acceleration at the impact six times higher than that of the nondisabled subjects (p < 0.001). Sitting with stimulation resulted in impact forces at initial contact with the seating surface averaging 1.4 times body weight and representing an average of twice the impact forces of the nondisabled subjects (p < 0.001). These results indicate a need for additional interventions to better control descent, minimize impact, and gently transition from standing to sitting to achieve a more natural movement and reduce the risk of injury.
Keywords: SCI; biomechanics; functional neuromuscular stimulation; impact force; neuroprosthesis; paralysis; spinal cord injury; stand-to-sit; upper-limb force; vertical acceleration.
Figures
Similar articles
-
Improving stand-to-sit maneuver for individuals with spinal cord injury.J Neuroeng Rehabil. 2016 Mar 15;13:27. doi: 10.1186/s12984-016-0137-6. J Neuroeng Rehabil. 2016. PMID: 26979386 Free PMC article.
-
Computation of the kinematics and the minimum peak joint moments of sit-to-stand movements.Biomed Eng Online. 2007 Jul 3;6:26. doi: 10.1186/1475-925X-6-26. Biomed Eng Online. 2007. PMID: 17608922 Free PMC article.
-
Simulation of functional neuromuscular stimulation assisted sit-to-stand movements.Biomed Sci Instrum. 2003;39:300-5. Biomed Sci Instrum. 2003. PMID: 12724910
-
Contributions to the understanding of gait control.Dan Med J. 2014 Apr;61(4):B4823. Dan Med J. 2014. PMID: 24814597 Review.
-
Upper extremity neuroprostheses using functional electrical stimulation.Baillieres Clin Neurol. 1995 Apr;4(1):57-75. Baillieres Clin Neurol. 1995. PMID: 7633785 Review. No abstract available.
Cited by
-
A muscle-driven approach to restore stepping with an exoskeleton for individuals with paraplegia.J Neuroeng Rehabil. 2017 May 30;14(1):48. doi: 10.1186/s12984-017-0258-6. J Neuroeng Rehabil. 2017. PMID: 28558835 Free PMC article.
-
Effect of high-fat diet on isometric, concentric and eccentric contractile performance of skeletal muscle isolated from female CD-1 mice.Exp Physiol. 2024 Jul;109(7):1163-1176. doi: 10.1113/EP091832. Epub 2024 May 9. Exp Physiol. 2024. PMID: 38723238 Free PMC article.
-
Rollator usage lets young individuals switch movement strategies in sit-to-stand and stand-to-sit tasks.Sci Rep. 2023 Oct 6;13(1):16901. doi: 10.1038/s41598-023-43401-6. Sci Rep. 2023. PMID: 37803010 Free PMC article.
-
Improving stand-to-sit maneuver for individuals with spinal cord injury.J Neuroeng Rehabil. 2016 Mar 15;13:27. doi: 10.1186/s12984-016-0137-6. J Neuroeng Rehabil. 2016. PMID: 26979386 Free PMC article.
-
Powered Lower-Limb Exoskeletons to Restore Gait for Individuals with Paraplegia - a Review.Case Orthop J. 2015;12(1):75-80. Case Orthop J. 2015. PMID: 28004009 Free PMC article.
References
-
- Mushahwar VK, Jacobs PL, Normann RA, Triolo RJ, Kleitman N. New functional electrical stimulation approaches to standing and walking. J Neural Eng. 2007;4(3):S181–97. http://dx.doi.org/10.1088/1741-2560/4/3/S05. - DOI - PubMed
-
- Triolo RJ, Bailey SN, Miller ME, Rohde LM, Anderson JS, Davis JA, Jr, Abbas JJ, DiPonio LA, Forrest GP, Gater DR, Jr, Yang LJ. Longitudinal performance of a surgically implanted neuroprosthesis for lower-extremity exercise, standing, and transfers after spinal cord injury. Arch Phys Med Rehabil. 2012;93(5):896–904. http://dx.doi.org/10.1016/j.apmr.2012.01.001. - DOI - PMC - PubMed
-
- Marsolais EB, Kobetic R. Development of a practical electrical stimulation system for restoring gait in the paralyzed patient. Clin Orthop Relat Res. 1988;(233):64–74. - PubMed
-
- Kobetic R, Marsolais EB. Synthesis of paraplegic gait with multichannel functional neuromuscular stimulation. IEEE Trans Rehabil Eng. 1994;2(2):66–79. http://dx.doi.org/10.1109/86.313148. - DOI
-
- Gallien P, Brissot R, Eyssette M, Tell L, Barat M, Wiart L, Petit H. Restoration of gait by functional electrical stimulation for spinal cord injured patients. Paraplegia. 1995;33(11):660–64. http://dx.doi.org/10.1038/sc.1995.138. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical