

The risk of hospitalization and modality failure with home dialysis
- PMID: 25786099
- PMCID: PMC4526768
- DOI: 10.1038/ki.2015.68
The risk of hospitalization and modality failure with home dialysis
Abstract
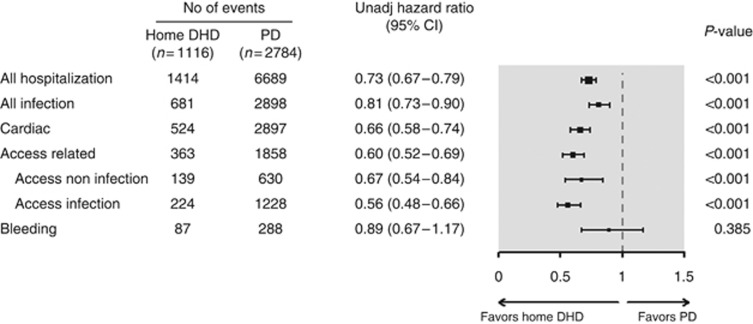
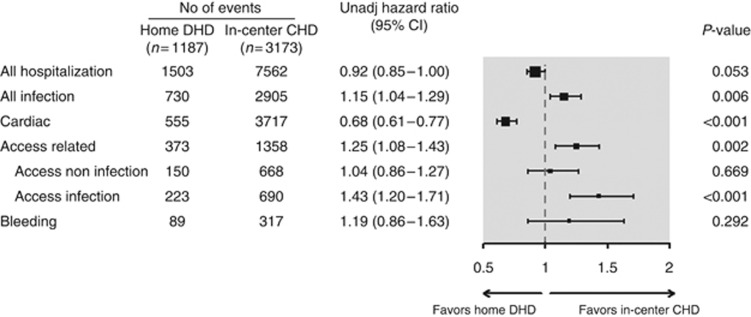
While home dialysis is being promoted, there are few comparative effectiveness studies of home-based modalities to guide patient decisions. To address this, we matched 1116 daily home hemodialysis (DHD) patients by propensity scores to 2784 contemporaneous USRDS patients receiving home peritoneal dialysis (PD), and compared hospitalization rates from cardiovascular, infectious, access-related or bleeding causes (prespecified composite), and modality failure risk. We performed similar analyses for 1187 DHD patients matched to 3173 USRDS patients receiving in-center conventional hemodialysis (CHD). The composite hospitalization rate was significantly lower with DHD than with PD (0.93 vs. 1.35/patient-year, hazard ratio=0.73 (95% CI=0.67-0.79)). DHD patients spent significantly fewer days in hospital than PD patients (5.2 vs. 9.2 days/patient-year), and significantly more DHD patients remained admission-free (52% DHD vs. 32% PD). In contrast, there was no significant difference in hospitalizations between DHD and CHD (DHD vs. CHD: 0.93 vs. 1.10/patient-year, hazard ratio 0.92 (0.85-1.00)). Cardiovascular hospitalizations were lower with DHD than with CHD (0.68 (0.61-0.77)), while infectious and access hospitalizations were higher (1.15 (1.04-1.29) and 1.25 (1.08-1.43), respectively). Significantly more PD than DHD patients switched back to in-center HD (44% vs. 15%; 3.4 (2.9-4.0)). In this prevalent cohort, home DHD was associated with fewer admissions and hospital days than PD, and a substantially lower risk of modality failure.
Figures
References
-
- Thodis ED, Oreopoulos DG. Home dialysis first: a new paradigm for new ESRD patients. J Nephrol. 2011;24:398–404. - PubMed
-
- Burkart J. Role of peritoneal dialysis in the era of the resurgence of home hemodialysis. Hemodial Int. 2008;12:S51–S54. - PubMed
-
- Burkart J. The future of peritoneal dialysis in the United States: optimizing its use. Clin J Am Soc Nephrol. 2009;4:S125–S131. - PubMed
-
- Chow J, Fortnum D, Moodie JA, et al. The HOME network: an Australian national initiative for home therapies. J Ren Care. 2013;39:56–61. - PubMed
-
- Heaf J. Underutilization of peritoneal dialysis. JAMA. 2004;291:740–742. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
