

Prevalence of chronic kidney disease in two major Indian cities and projections for associated cardiovascular disease
- PMID: 25786102
- PMCID: PMC4490055
- DOI: 10.1038/ki.2015.58
Prevalence of chronic kidney disease in two major Indian cities and projections for associated cardiovascular disease
Abstract
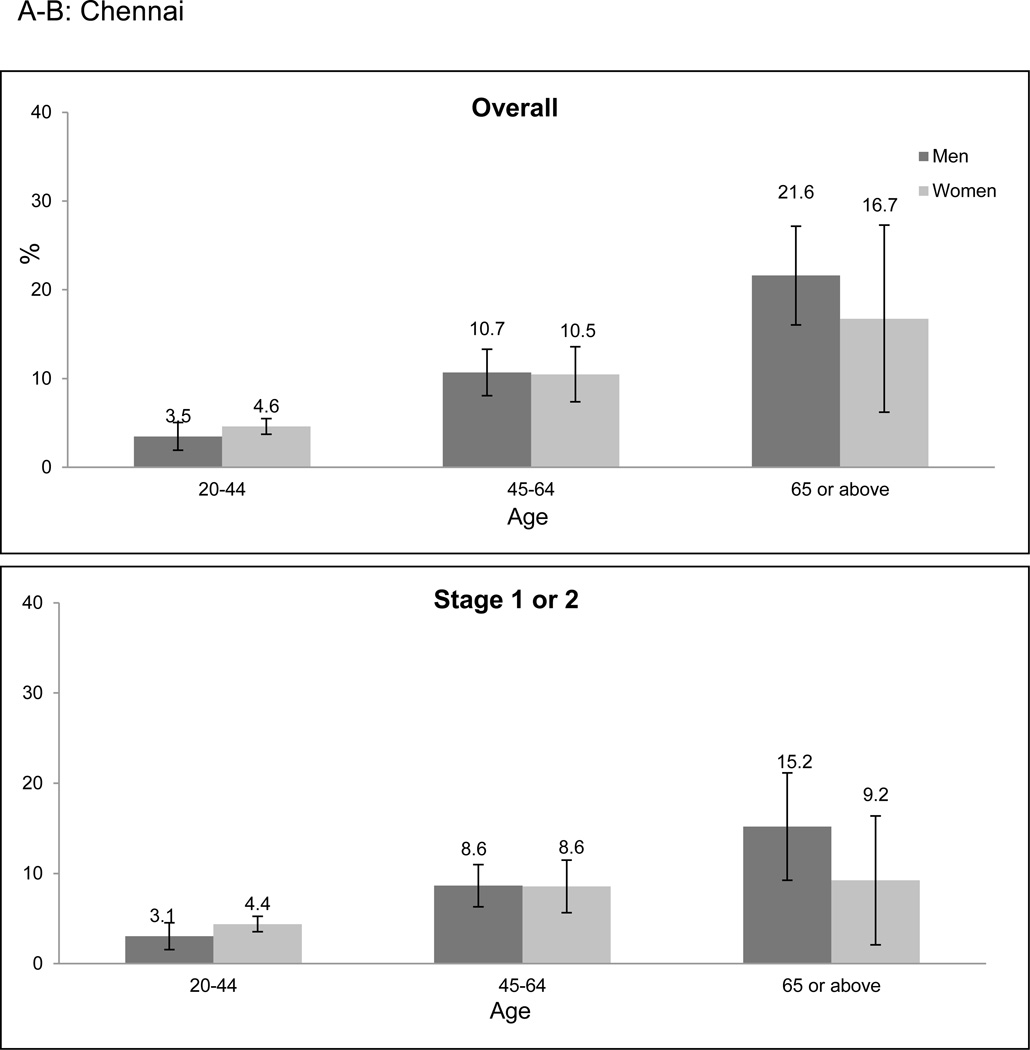
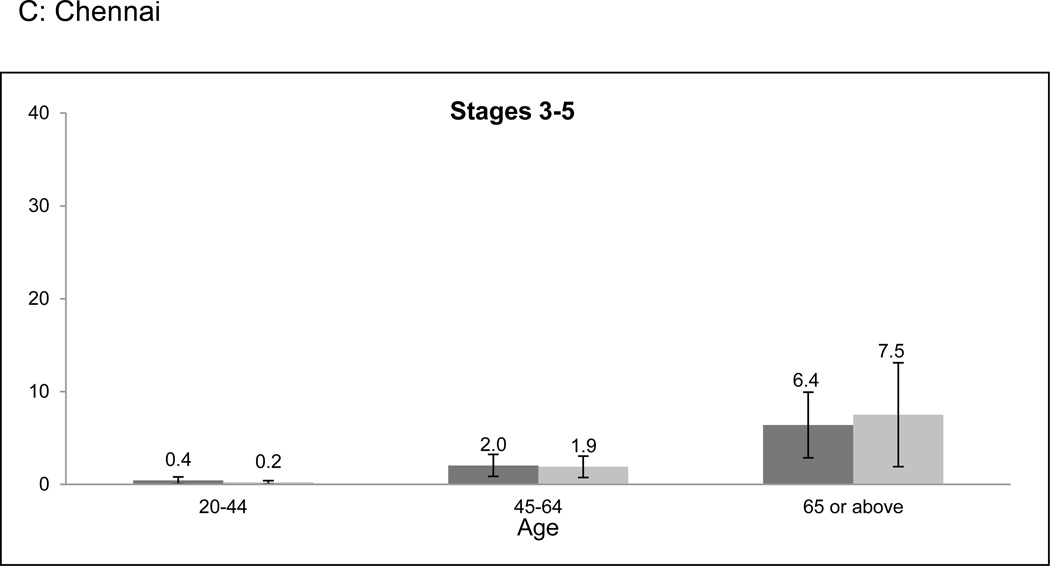
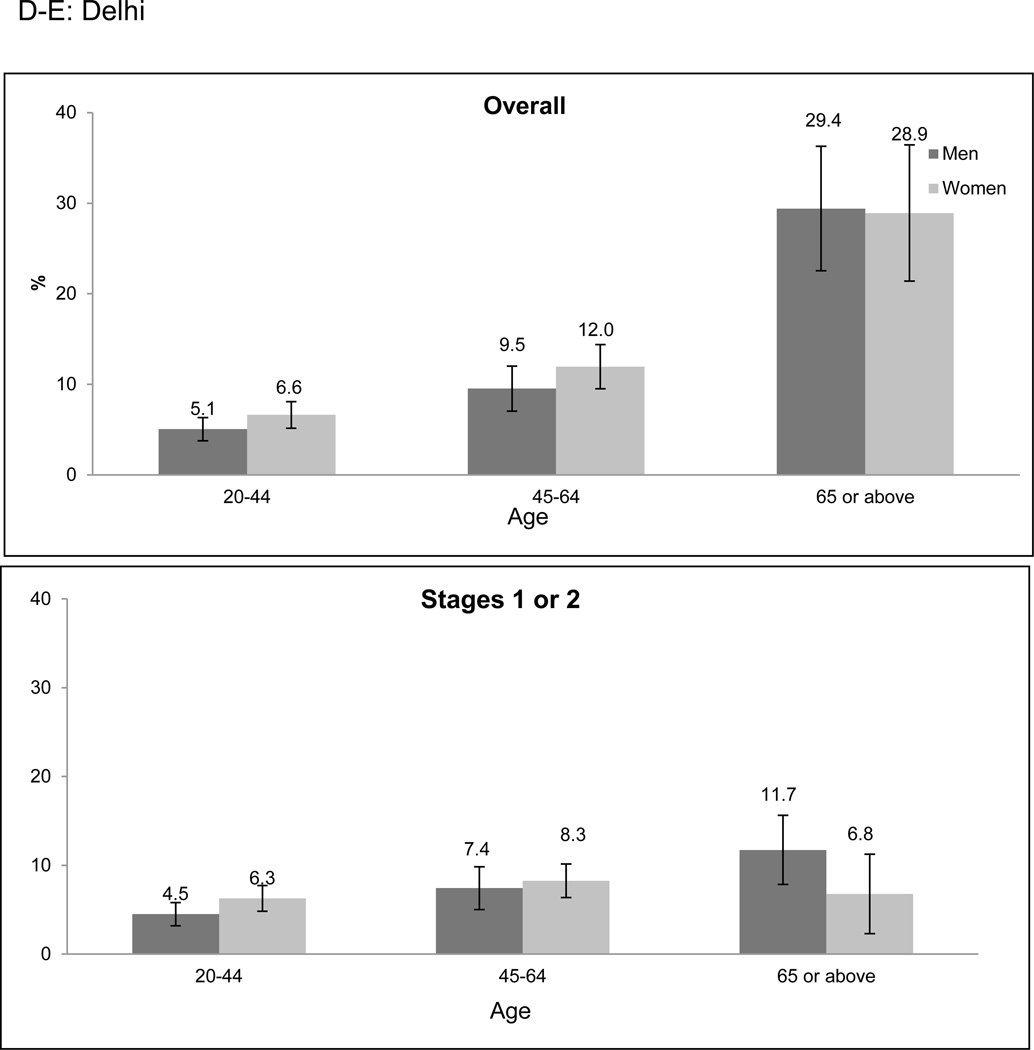
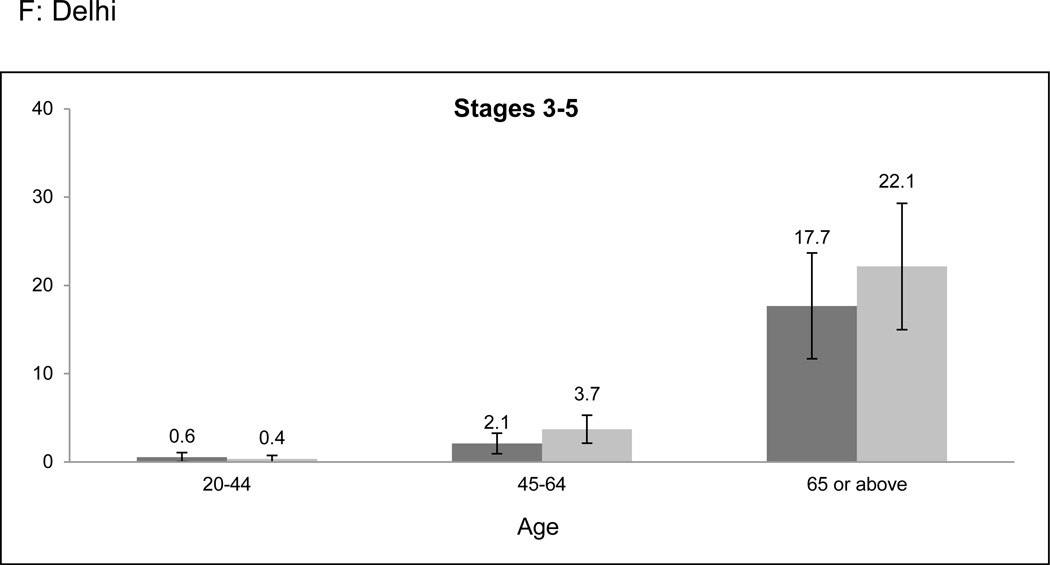
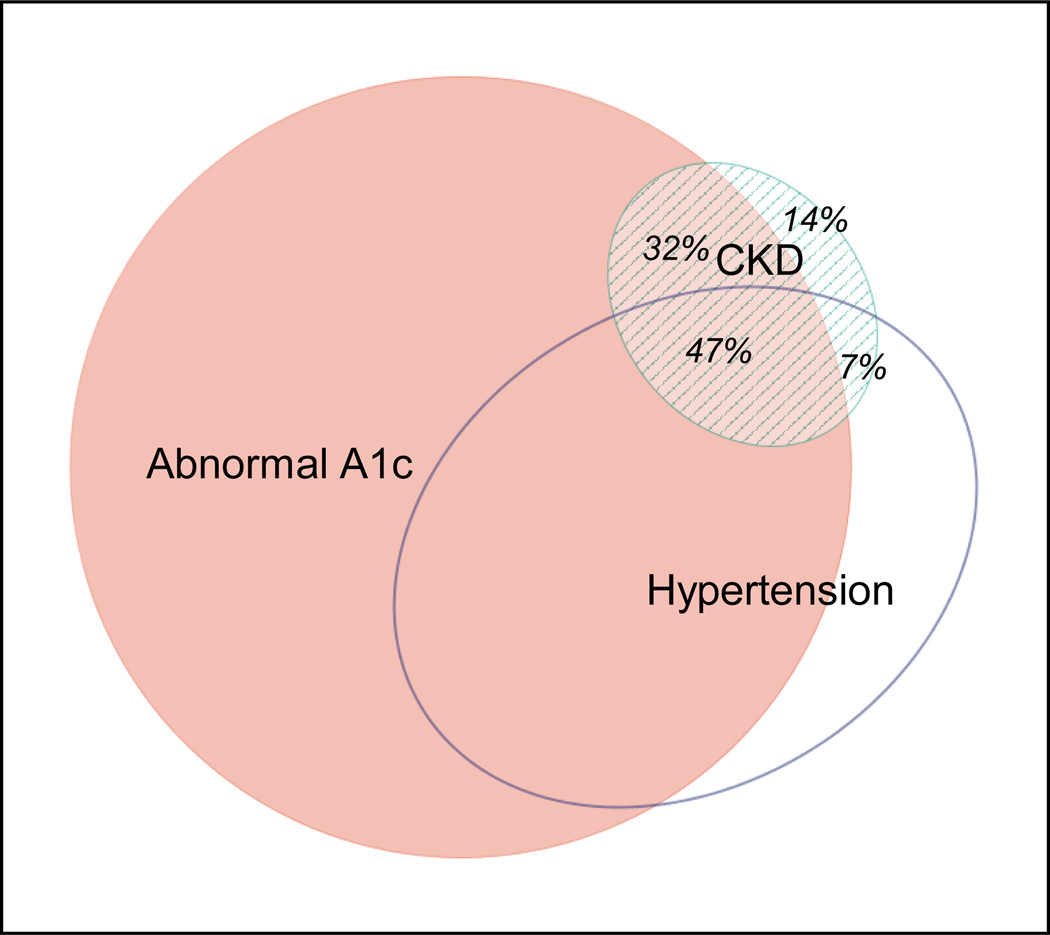
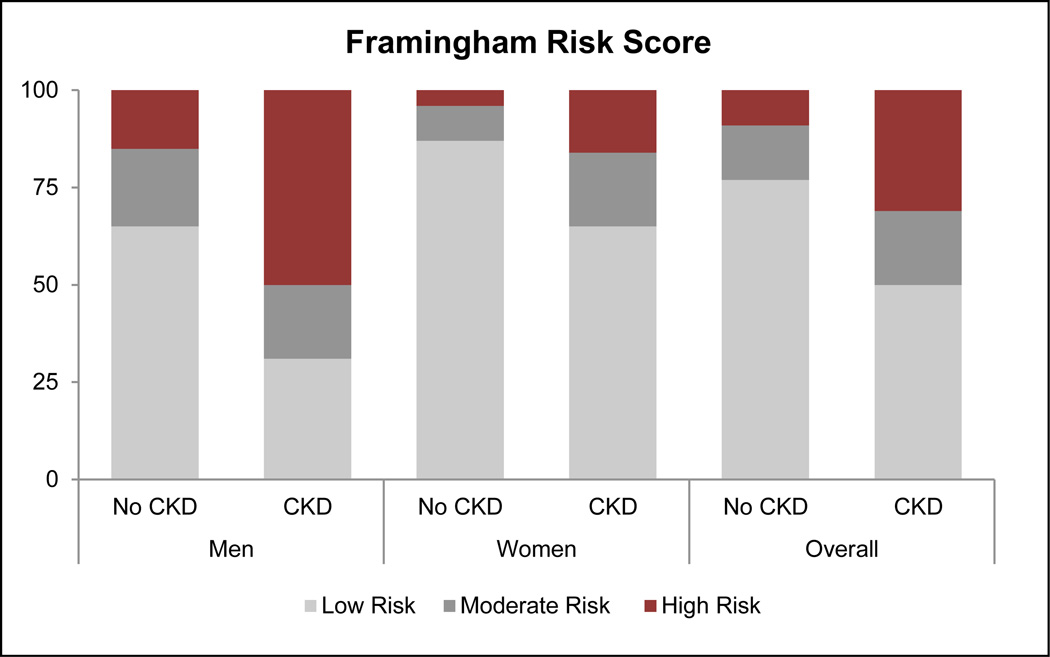
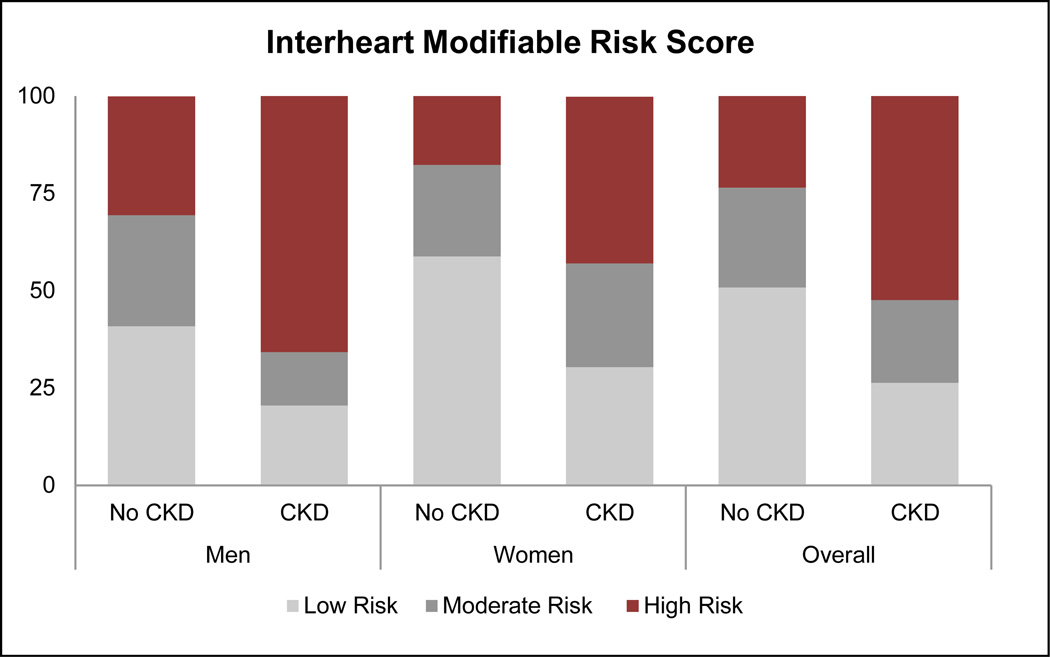
India is experiencing an alarming rise in the burden of noncommunicable diseases, but data on the incidence of chronic kidney disease (CKD) are sparse. Using the Center for Cardiometabolic Risk Reduction in South Asia surveillance study (a population-based survey of Delhi and Chennai, India) we estimated overall, and age-, sex-, city-, and diabetes-specific prevalence of CKD, and defined the distribution of the study population by the Kidney Disease Improving Global Outcomes (KDIGO) classification scheme. The likelihood of cardiovascular events in participants with and without CKD was estimated by the Framingham and Interheart Modifiable Risk Scores. Of the 12,271 participants, 80% had complete data on serum creatinine and albuminuria. The prevalence of CKD and albuminuria, age standardized to the World Bank 2010 world population, was 8.7% (95% confidence interval: 7.9-9.4%) and 7.1% (6.4-7.7%), respectively. Nearly 80% of patients with CKD had an abnormally high hemoglobin A1c (5.7 and above). Based on KDIGO guidelines, 6.0, 1.0, and 0.5% of study participants are at moderate, high, or very high risk for experiencing CKD-associated adverse outcomes. The cardiovascular risk scores placed a greater proportion of patients with CKD in the high-risk categories for experiencing cardiovascular events when compared with participants without CKD. Thus, 1 in 12 individuals living in two of India's largest cities have evidence of CKD, with features that put them at high risk for adverse outcomes.
Conflict of interest statement
Disclosures/Conflict of Interest
The authors have no conflicts of interest to declare.
Figures
References
-
- Prentice AM. The emerging epidemic of obesity in developing countries. International journal of epidemiology. 2006;35(1):93–99. - PubMed
-
- Hossain P, Kawar B, El Nahas M. Obesity and diabetes in the developing world--a growing challenge. The New England journal of medicine. 2007;356(3):213–215. - PubMed
-
- Barsoum RS. Chronic kidney disease in the developing world. The New England journal of medicine. 2006;354(10):997–999. - PubMed
-
- Matsushita K, van der Velde M, Astor BC, Woodward M, Levey AS, et al. Chronic Kidney Disease Prognosis C. Association of estimated glomerular filtration rate and albuminuria with all-cause and cardiovascular mortality in general population cohorts: a collaborative meta-analysis. Lancet. 2010;375(9731):2073–2081. - PMC - PubMed
-
- USRDS 2013: Atlas of End-Stage Renal Disease [Internet] Bethesda: National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases; 2013. [cited January 7 2013].
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
