

A mechanistic tumor penetration model to guide antibody drug conjugate design
- PMID: 25786126
- PMCID: PMC4364906
- DOI: 10.1371/journal.pone.0118977
A mechanistic tumor penetration model to guide antibody drug conjugate design
Abstract
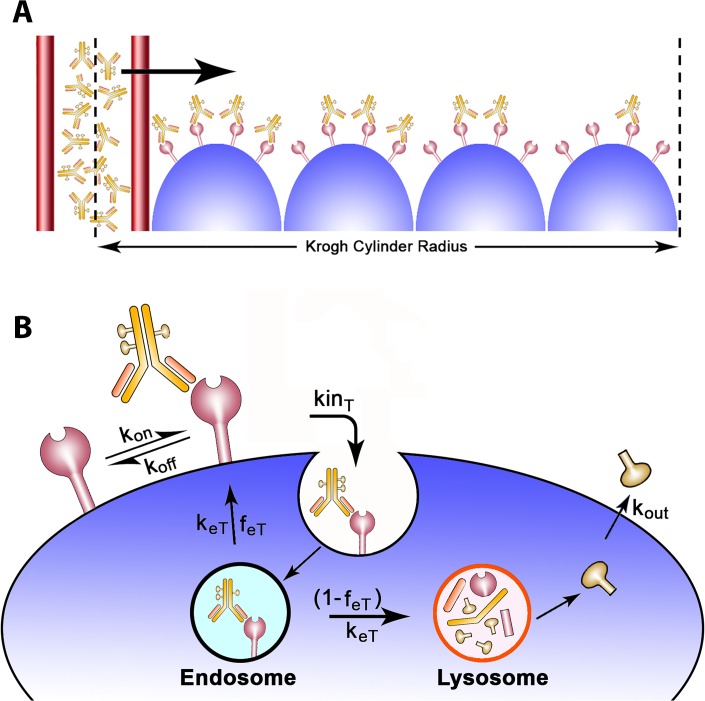
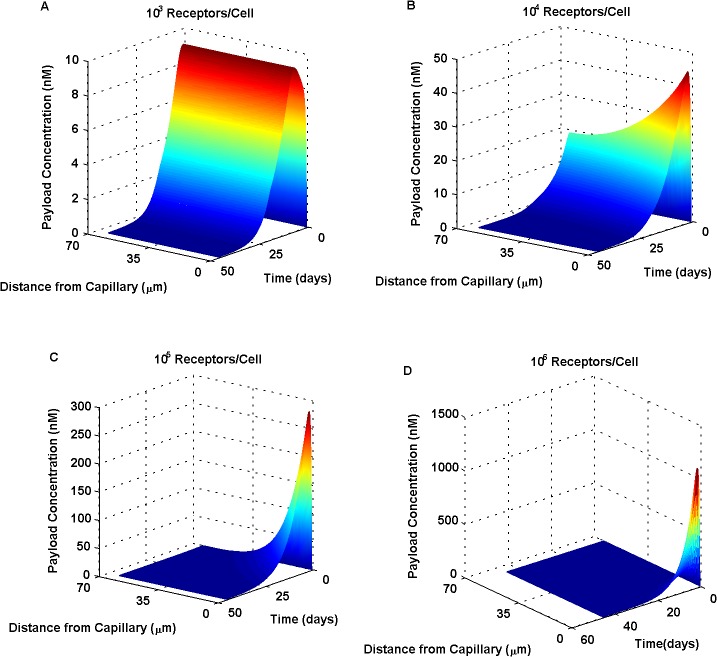
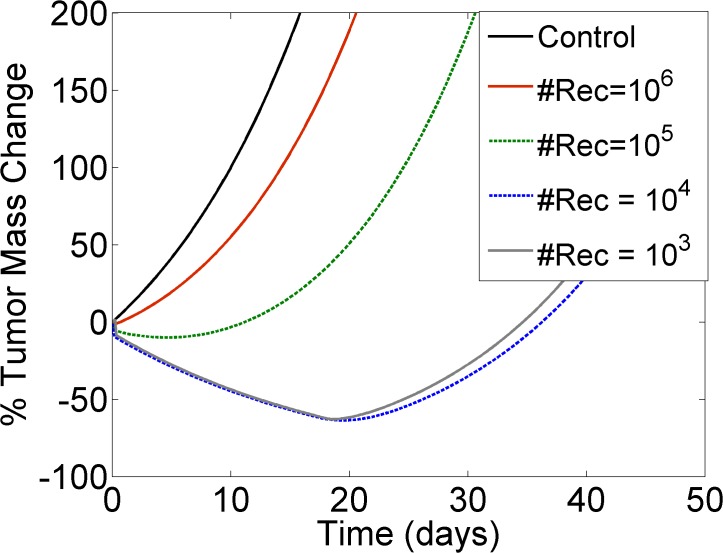
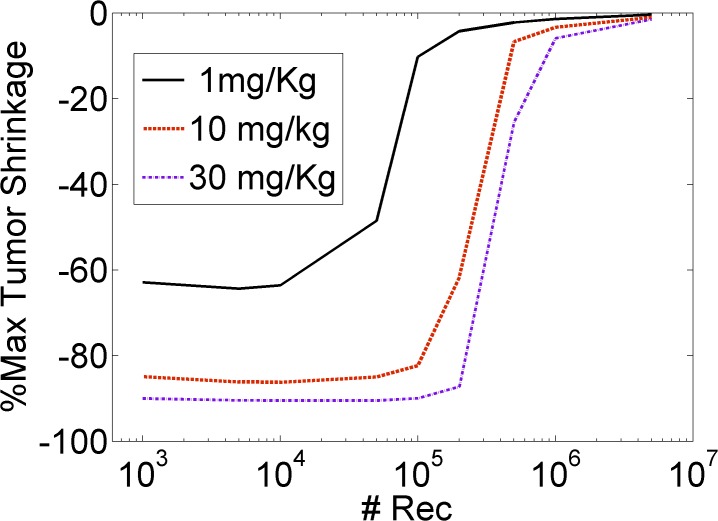
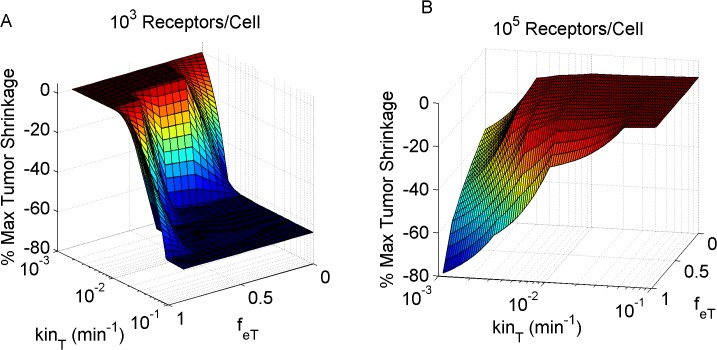
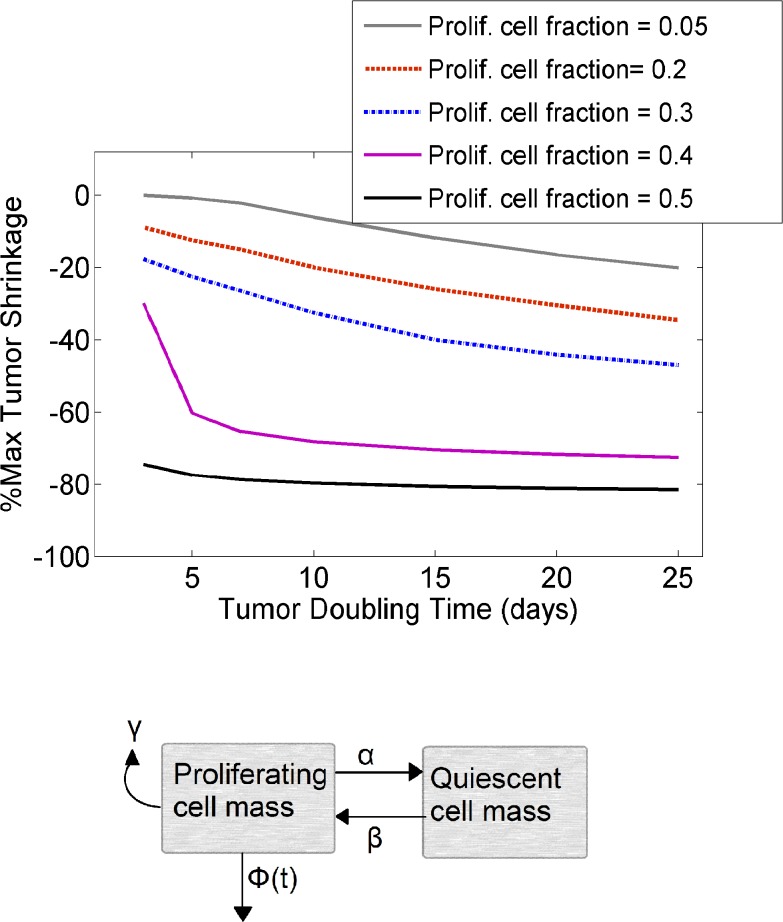
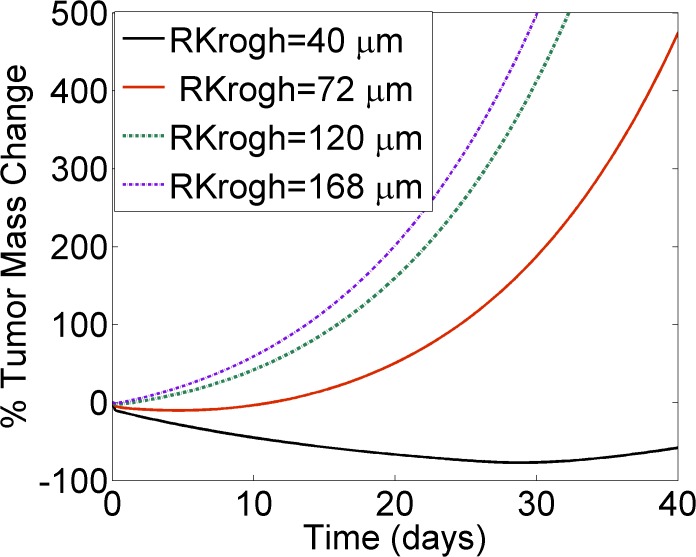
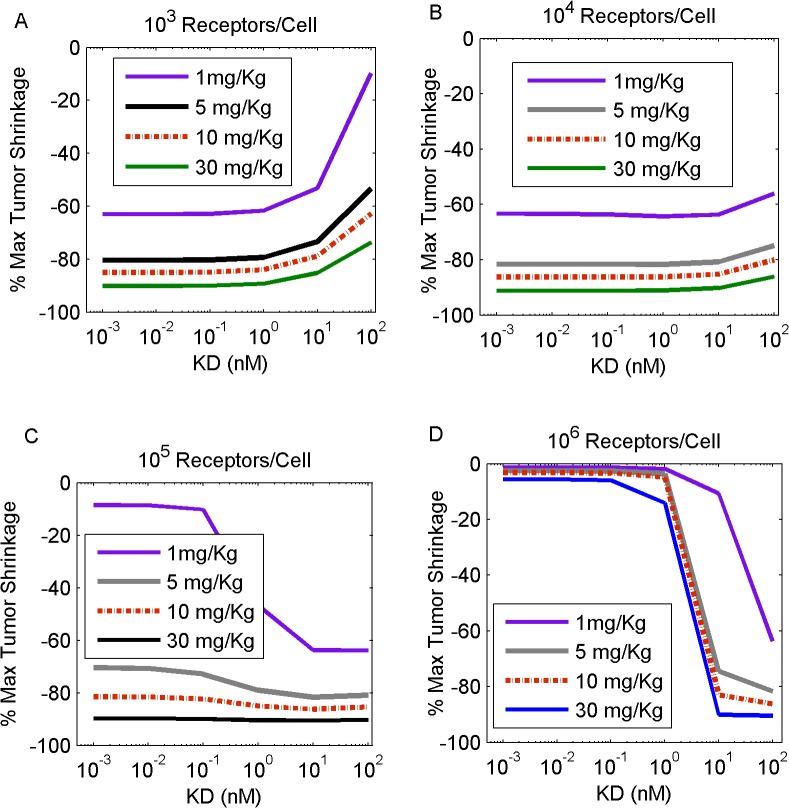
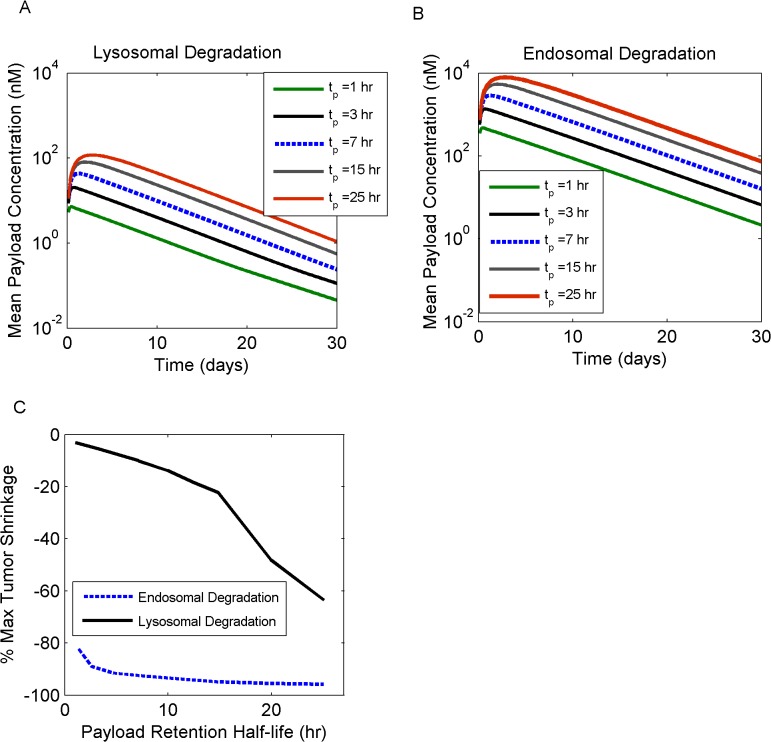
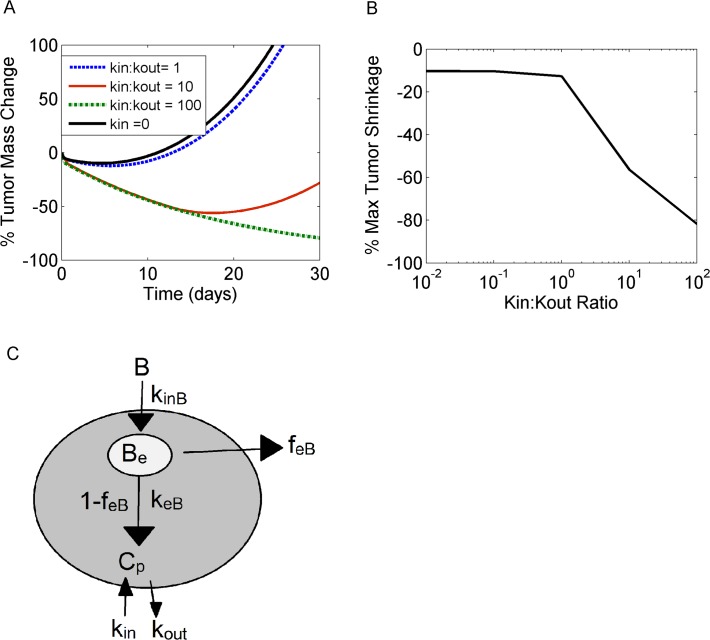
Antibody drug conjugates (ADCs) represent novel anti-cancer modalities engineered to specifically target and kill tumor cells expressing corresponding antigens. Due to their large size and their complex kinetics, these therapeutic agents often face heterogeneous distributions in tumors, leading to large untargeted regions that escape therapy. We present a modeling framework which includes the systemic distribution, vascular permeability, interstitial transport, as well as binding and payload release kinetics of ADC-therapeutic agents in mouse xenografts. We focused, in particular, on receptor dynamics such as endocytic trafficking mechanisms within cancer cells, to simulate their impact on tumor mass shrinkage upon ADC administration. Our model identified undesirable tumor properties that can impair ADC tissue homogeneity, further compromising ADC success, and explored ADC design optimization scenarios to counteract upon such unfavorable intrinsic tumor tissue attributes. We further demonstrated the profound impact of cytotoxic payload release mechanisms and the role of bystander killing effects on tumor shrinkage. This model platform affords a customizable simulation environment which can aid with experimental data interpretation and the design of ADC therapeutic treatments.
Conflict of interest statement
Figures
References
-
- Burris HA, Rugo HS, Vukelja SJ, Vogel CL, Borson RA, Limentani S, et al. Phase II Study of the Antibody Drug Conjugate Trastuzumab-DM1 for the Treatment of Human Epidermal Growth Factor Receptor 2 (HER2)-Positive Breast Cancer After Prior HER2-Directed Therapy. Journal of Clinical Oncology. 2011;29(4):398–405. 10.1200/JCO.2010.29.5865 - DOI - PubMed
-
- Krop I, LoRusso P, Miller KD, Modi S, Yardley D, Rodriguez G, et al. A Phase II Study of Trastuzumab-DM1 (T-DM1), a Novel HER2 Antibody-Drug Conjugate, in Patients Previously Treated with Lapatinib, Trastuzumab, and Chemotherapy. Cancer Research. 2009;69(24):795S–S.
-
- Younes A, Gopal AK, Smith SE, Ansell SM, Rosenblatt JD, Savage KJ, et al. Results from a pivotal phase II study of brentuximab vedotin (SGN-35) in patients with relapsed or refractory Hodgkin lymphoma (HL). ASCO Meeting Abstracts 2011. p. (15 suppl; abstr 8031).
-
- Wadleigh M, Richardson PG, Zahrieh D, Lee SJ, Cutler C, Ho V, et al. Prior gemtuzumab ozogamicin exposure significantly increases the risk of veno-occlusive disease in patients who undergo myeloablative allogeneic stem cell transplantation. Blood. 2003;102(5):1578–82. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
