

Benefits and Risks of Extended Duration Dual Antiplatelet Therapy After PCI in Patients With and Without Acute Myocardial Infarction
- PMID: 25787199
- PMCID: PMC4678101
- DOI: 10.1016/j.jacc.2015.03.003
Benefits and Risks of Extended Duration Dual Antiplatelet Therapy After PCI in Patients With and Without Acute Myocardial Infarction
Abstract
Background: The benefits and risks of prolonged dual antiplatelet therapy may be different for patients with acute myocardial infarction (MI) compared with more stable presentations.
Objectives: This study sought to assess the benefits and risks of 30 versus 12 months of dual antiplatelet therapy among patients undergoing coronary stent implantation with and without MI.
Methods: The Dual Antiplatelet Therapy Study, a randomized double-blind, placebo-controlled trial, compared 30 versus 12 months of dual antiplatelet therapy after coronary stenting. The effect of continued thienopyridine on ischemic and bleeding events among patients initially presenting with versus without MI was assessed. The coprimary endpoints were definite or probable stent thrombosis and major adverse cardiovascular and cerebrovascular events (MACCE). The primary safety endpoint was GUSTO (Global Utilization of Streptokinase and Tissue Plasminogen Activator for Occluded Arteries) moderate or severe bleeding.
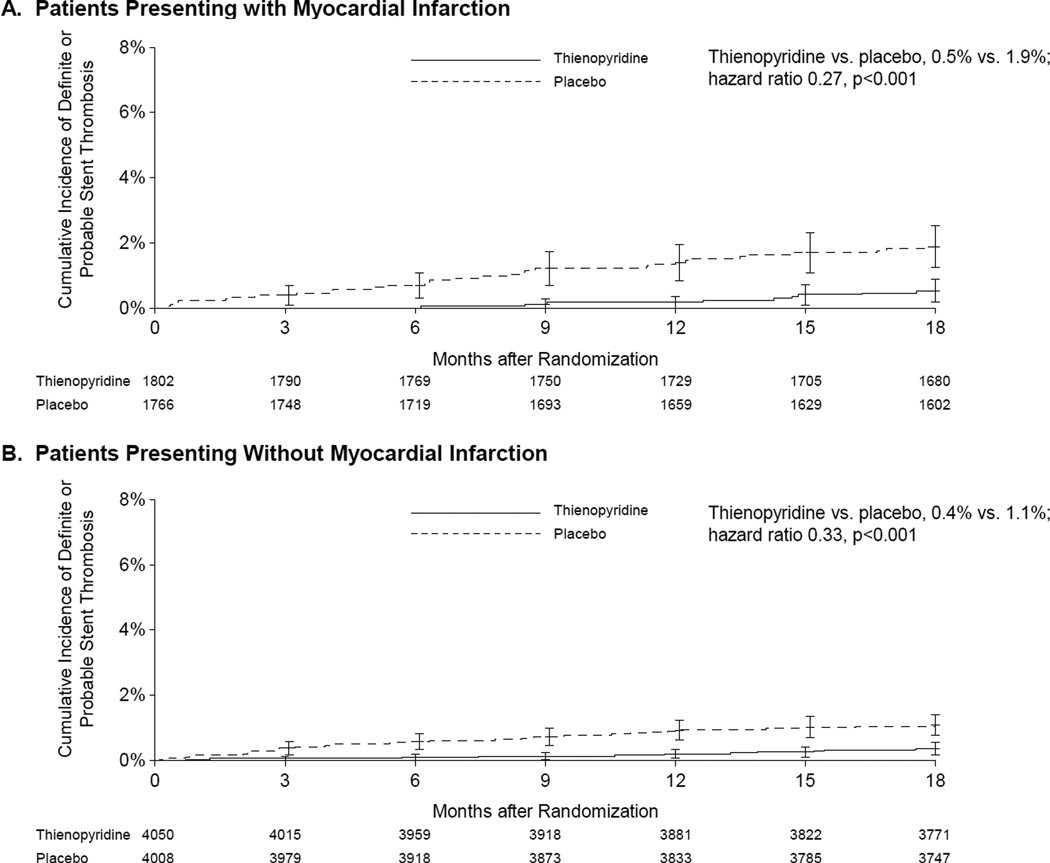
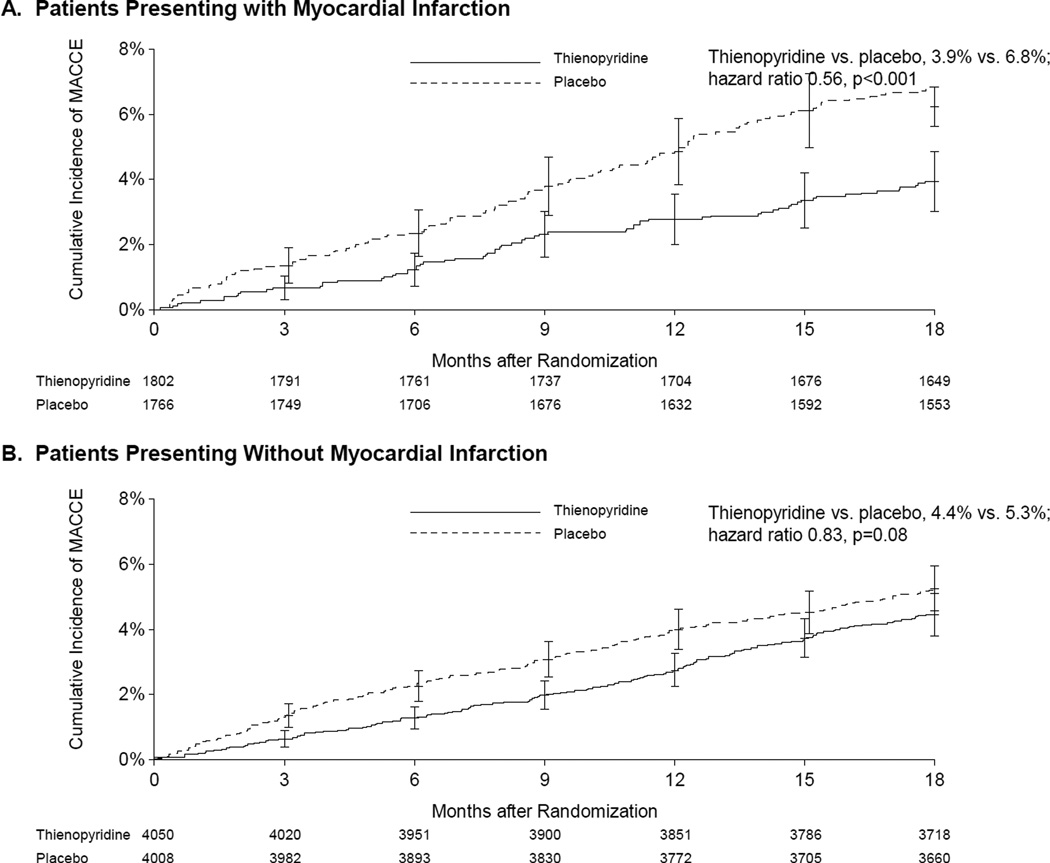
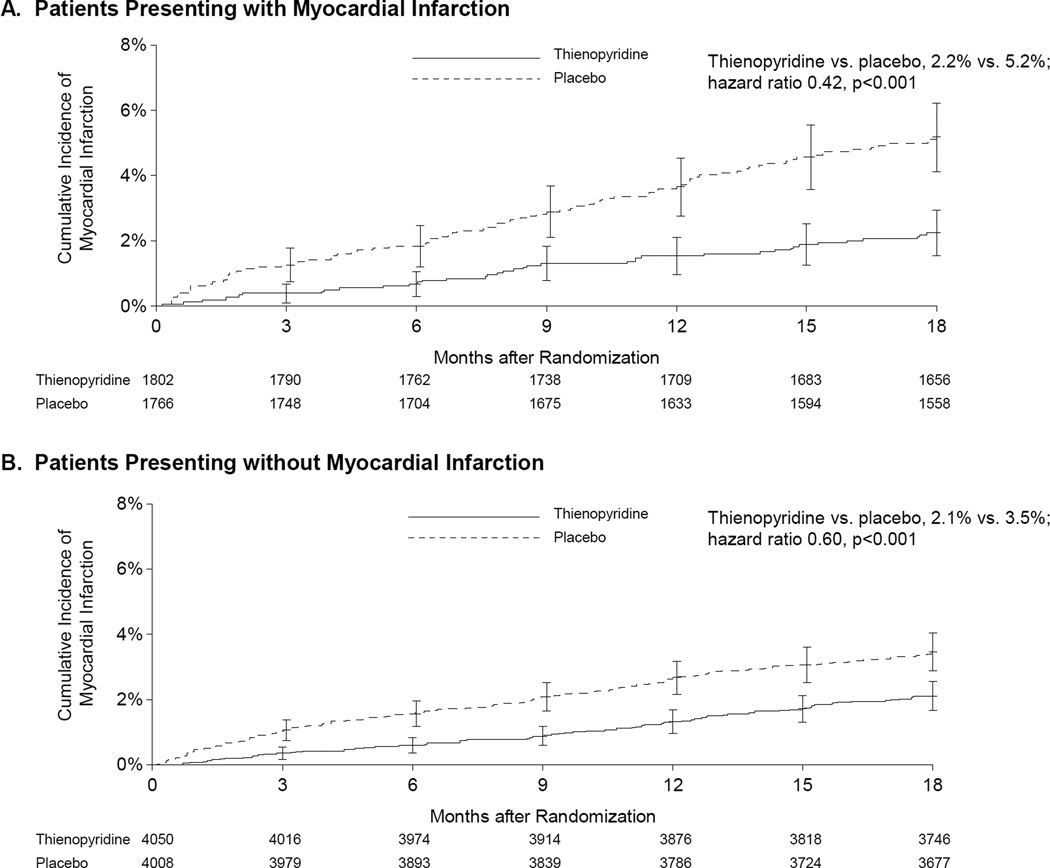
Results: Of 11,648 randomized patients (9,961 treated with drug-eluting stents, 1,687 with bare-metal stents), 30.7% presented with MI. Between 12 and 30 months, continued thienopyridine reduced stent thrombosis compared with placebo in patients with and without MI at presentation (MI group, 0.5% vs. 1.9%, p < 0.001; no MI group, 0.4% vs. 1.1%, p < 0.001; interaction p = 0.69). The reduction in MACCE for continued thienopyridine was greater for patients with MI (3.9% vs. 6.8%; p < 0.001) compared with those with no MI (4.4% vs. 5.3%; p = 0.08; interaction p = 0.03). In both groups, continued thienopyridine reduced MI (2.2% vs. 5.2%, p < 0.001 for MI; 2.1% vs. 3.5%, p < 0.001 for no MI; interaction p = 0.15) but increased bleeding (1.9% vs. 0.8%, p = 0.005 for MI; 2.6% vs. 1.7%, p = 0.007 for no MI; interaction p = 0.21).
Conclusions: Compared with 12 months of therapy, 30 months of dual antiplatelet therapy reduced the risk of stent thrombosis and MI in patients with and without MI, and increased bleeding. (The Dual Antiplatelet Therapy Study [The DAPT Study]; NCT00977938).
Keywords: acute coronary syndromes; antiplatelet therapy; myocardial infarction; percutaneous coronary intervention; randomized clinical trial.
Copyright © 2015 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Figures

Comment in
-
Double antiplatelet therapy duration: standardize or personalize?J Am Coll Cardiol. 2015 May 26;65(20):2222-4. doi: 10.1016/j.jacc.2015.03.541. J Am Coll Cardiol. 2015. PMID: 25998667 No abstract available.
-
Impact of Clinical Presentation on Dual Antiplatelet Therapy Duration: Let's Re-Evaluate Our Priorities.J Am Coll Cardiol. 2015 Sep 8;66(10):1203-4. doi: 10.1016/j.jacc.2015.05.080. J Am Coll Cardiol. 2015. PMID: 26338004 No abstract available.
-
Reply: Impact of Clinical Presentation on Dual Antiplatelet Therapy Duration: Let's Re-Evaluate Our Priorities.J Am Coll Cardiol. 2015 Sep 8;66(10):1204-5. doi: 10.1016/j.jacc.2015.06.1331. J Am Coll Cardiol. 2015. PMID: 26338005 No abstract available.
-
Analysis of Dual Antiplatelet Therapy.J Am Coll Cardiol. 2015 Nov 3;66(18):2055-2056. doi: 10.1016/j.jacc.2015.06.1357. J Am Coll Cardiol. 2015. PMID: 26516011 No abstract available.
-
Reply: Analysis of Dual Antiplatelet Therapy.J Am Coll Cardiol. 2015 Nov 3;66(18):2056. doi: 10.1016/j.jacc.2015.08.855. J Am Coll Cardiol. 2015. PMID: 26516012 No abstract available.
References
-
- Jernberg T, Hasvold P, Henriksson M, Hjelm H, Thuresson M, Janzon M. Cardiovascular risk in post-myocardial infarction patients: nationwide real world data demonstrate the importance of a long-term perspective. European heart journal. 2015 [epub ahead of print] - PubMed
-
- van Werkum JW, Heestermans AA, Zomer AC, et al. Predictors of coronary stent thrombosis: the Dutch Stent Thrombosis Registry. Journal of the American College of Cardiology. 2009;53:1399–1409. - PubMed
-
- Authors/Task Force m. Windecker S, Kolh P, et al. 2014 ESC/EACTS Guidelines on myocardial revascularization: The Task Force on Myocardial Revascularization of the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS)Developed with the special contribution of the European Association of Percutaneous Cardiovascular Interventions (EAPCI) European heart journal. 2014;35:2541–2619. - PubMed
-
- Levine GN, Bates ER, Blankenship JC, et al. 2011 ACCF/AHA/SCAI Guideline for Percutaneous Coronary Intervention. A report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines and the Society for Cardiovascular Angiography and Interventions. Journal of the American College of Cardiology. 2011;58:e44–e122. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
