

Impact of stage migration and practice changes on high-risk prostate cancer: results from patients treated with radical prostatectomy over the last two decades
- PMID: 25787671
- PMCID: PMC5160041
- DOI: 10.1111/bju.13125
Impact of stage migration and practice changes on high-risk prostate cancer: results from patients treated with radical prostatectomy over the last two decades
Abstract
Objective: To evaluate the impact of year of surgery on clinical, pathological and oncological outcomes of patients with high-risk prostate cancer.
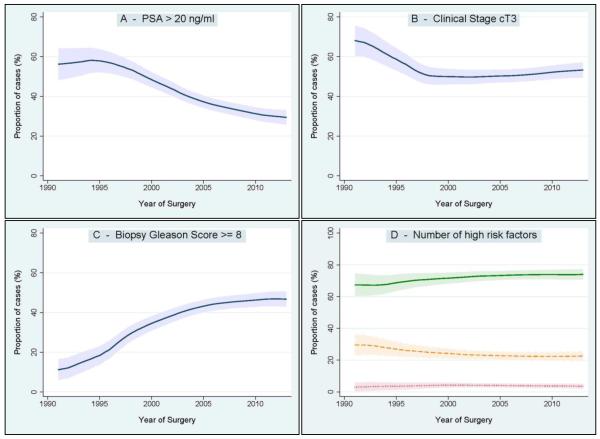
Patients and methods: We evaluated 1 033 patients with clinically high-risk prostate cancer, defined as the presence of at least one of the following risk factors: preoperative prostate-specific antigen (PSA) level >20 ng/mL, and/or clinical stage ≥T3, and/or biopsy Gleason score ≥8. Patients were treated between 1990 and 2013 at a single institution. The year-by-year trends in clinical and pathological characteristics were examined. Multivariable Cox regression analysis was used to test the relationship between year of surgery and oncological outcomes.
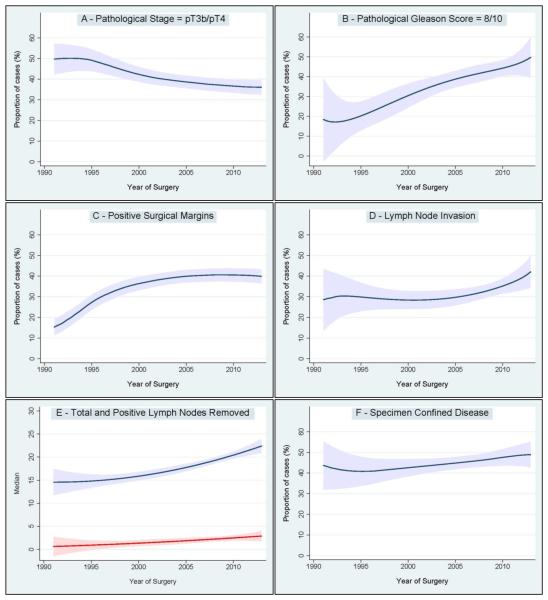
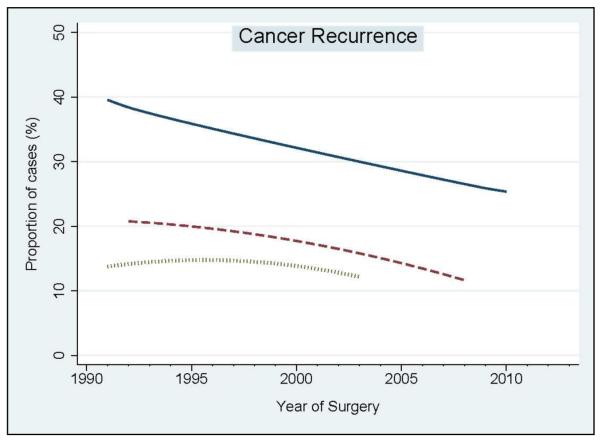
Results: We observed a decrease over time in the proportion of patients with high-risk disease (preoperative PSA >20 ng/mL or clinical stage cT3). A trend in the opposite direction was seen for biopsy Gleason score ≥8 tumours. We observed a considerable increase in the median number of lymph nodes removed, which was associated with an increased rate of lymph node invasion (LNI). On multivariable Cox regression analysis, year of surgery was associated with a reduced risk of biochemical recurrence (hazard ratio [HR] per 5-year interval 0.90, 95% confidence interval [CI] 0.84-0.96; P = 0.01) and distant metastasis (HR per 5-year interval 0.91, 95% CI 0.83-0.99; P = 0.039), after adjusting for age, preoperative PSA, pathological stage, LNI, surgical margin status, and pathological Gleason score.
Conclusions: In this single-centre study, an increased diagnosis of localized and less extensive high-grade prostate cancer was observed over the last two decades. Patients with high-risk disease who were selected for radical prostatectomy showed better cancer control over time. Better definitions of what constitutes high-risk prostate cancer among contemporary patients are needed.
Keywords: cancer recurrence; high risk; prostate cancer; radical prostatectomy; stage migration.
© 2015 The Authors BJU International © 2015 BJU International Published by John Wiley & Sons Ltd.
Figures
Similar articles
-
The Role of Prostate-specific Antigen Persistence After Radical Prostatectomy for the Prediction of Clinical Progression and Cancer-specific Mortality in Node-positive Prostate Cancer Patients.Eur Urol. 2016 Jun;69(6):1142-8. doi: 10.1016/j.eururo.2015.12.010. Epub 2015 Dec 31. Eur Urol. 2016. PMID: 26749093
-
Radical prostatectomy represents an effective treatment in patients with specimen-confined high pathological Gleason score prostate cancer.BJU Int. 2013 May;111(5):723-30. doi: 10.1111/j.1464-410X.2012.11114.x. Epub 2012 Apr 4. BJU Int. 2013. PMID: 22487441
-
Oncological control after radical prostatectomy in men with clinical T3 prostate cancer: a single-centre experience.BJU Int. 2009 May;103(9):1173-8; discussion 1178. doi: 10.1111/j.1464-410X.2008.08208.x. Epub 2008 Nov 25. BJU Int. 2009. PMID: 19040530
-
Long-term oncological outcomes after laparoscopic radical prostatectomy.BJU Int. 2013 Feb;111(2):271-80. doi: 10.1111/j.1464-410X.2012.11317.x. Epub 2012 Jul 3. BJU Int. 2013. PMID: 22757970 Review.
-
Radical Prostatectomy for High-risk Localized or Node-Positive Prostate Cancer: Removing the Primary.Curr Urol Rep. 2017 Jul;18(7):53. doi: 10.1007/s11934-017-0703-x. Curr Urol Rep. 2017. PMID: 28589400 Review.
Cited by
-
Biochemical recurrence-free survival and pathological outcomes after radical prostatectomy for high-risk prostate cancer.BMC Urol. 2016 Jun 8;16(1):26. doi: 10.1186/s12894-016-0146-6. BMC Urol. 2016. PMID: 27267988 Free PMC article.
-
Artificial Intelligence Combined With Big Data to Predict Lymph Node Involvement in Prostate Cancer: A Population-Based Study.Front Oncol. 2021 Oct 14;11:763381. doi: 10.3389/fonc.2021.763381. eCollection 2021. Front Oncol. 2021. PMID: 34722318 Free PMC article.
-
Relative impact of lymph-node metastasis and seminal vesical invasion on oncologic outcomes following radical prostatectomy.Prostate Cancer Prostatic Dis. 2024 Dec;27(4):674-679. doi: 10.1038/s41391-023-00724-9. Epub 2023 Sep 15. Prostate Cancer Prostatic Dis. 2024. PMID: 37714961
-
Clinical stage provides useful prognostic information even after pathological stage is known for prostate cancer in the PSA era.PLoS One. 2020 Jun 11;15(6):e0234391. doi: 10.1371/journal.pone.0234391. eCollection 2020. PLoS One. 2020. PMID: 32525914 Free PMC article.
-
The Role of Radiotherapy After Radical Prostatectomy in Patients with Prostate Cancer.Curr Oncol Rep. 2015 Dec;17(12):53. doi: 10.1007/s11912-015-0478-5. Curr Oncol Rep. 2015. PMID: 26449841 Review.
References
-
- D'Amico AV, Whittington R, Malkowicz SB, Schultz D, Blank K, Broderick GA, et al. Biochemical outcome after radical prostatectomy, external beam radiation therapy, or interstitial radiation therapy for clinically localized prostate cancer. Jama. 1998;280:969–74. - PubMed
-
- NCCN Clinical Practice Guidelines in Oncology [Accessed 04/01/2015];Prostate cancer. 2015 2014:1–98. Available at http://www.nccn.org/professionals/physician_gls/pdf/prostatepdf.
-
- Bastian PJ, Bellmunt J, Bolla M, Joniau S, van der Kwast T, Mason M, et al. EAU Guidelines on Prostate Cancer. Part 1: Screening, Diagnosis, and Local Treatment with Curative Intent—Update 2013. Eur Urol. 2014;65:124–37. - PubMed
-
- Hodgson D, Warde P, Gospodarowicz M. The management of locally advanced prostate cancer. Urologic Oncology: Seminars and Original Investigations. 1998;4:3–12. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
