

CD4 enumeration technologies: a systematic review of test performance for determining eligibility for antiretroviral therapy
- PMID: 25790185
- PMCID: PMC4366094
- DOI: 10.1371/journal.pone.0115019
CD4 enumeration technologies: a systematic review of test performance for determining eligibility for antiretroviral therapy
Abstract
Background: Measurement of CD4+ T-lymphocytes (CD4) is a crucial parameter in the management of HIV patients, particularly in determining eligibility to initiate antiretroviral treatment (ART). A number of technologies exist for CD4 enumeration, with considerable variation in cost, complexity, and operational requirements. We conducted a systematic review of the performance of technologies for CD4 enumeration.
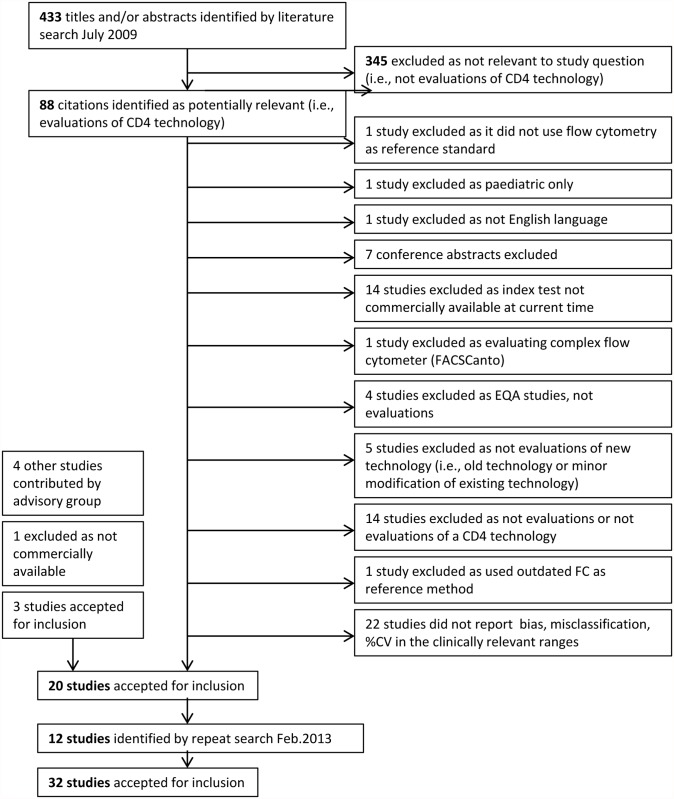
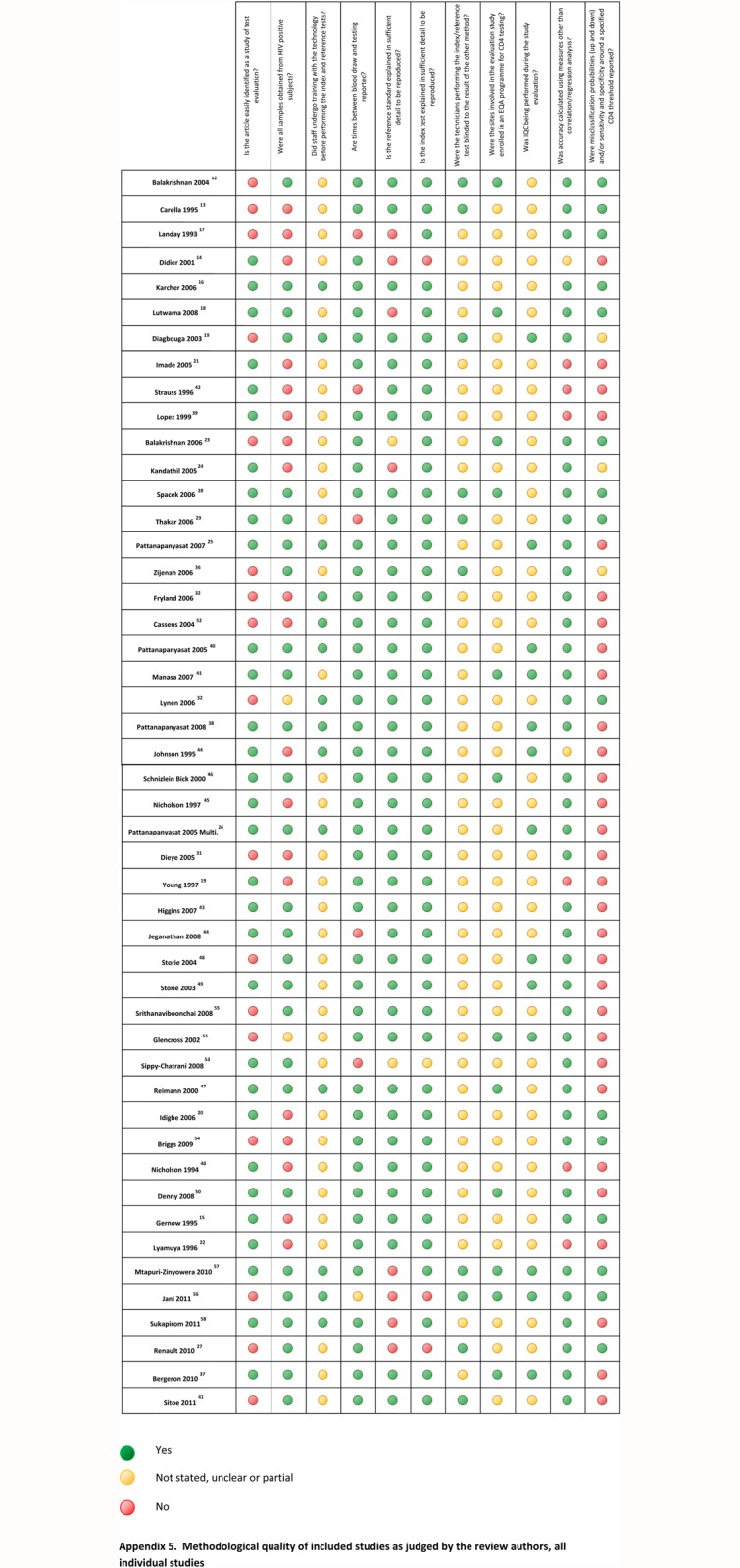
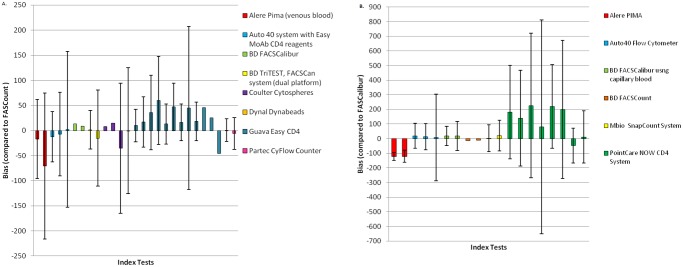
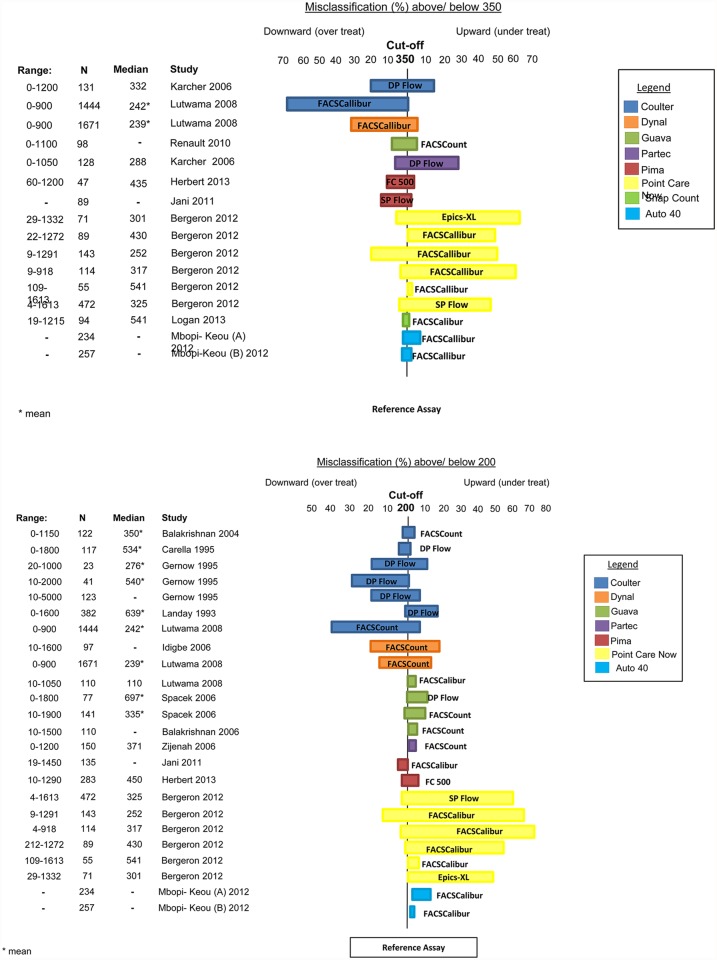
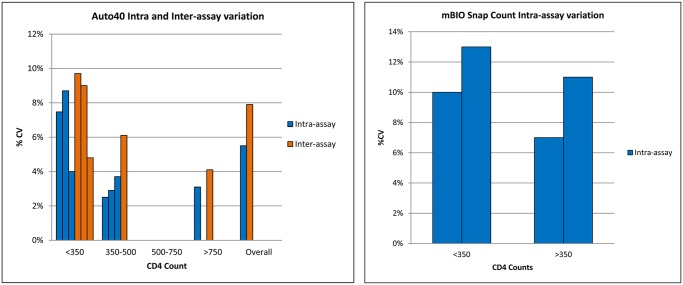
Methods and findings: Studies were identified by searching electronic databases MEDLINE and EMBASE using a pre-defined search strategy. Data on test accuracy and precision included bias and limits of agreement with a reference standard, and misclassification probabilities around CD4 thresholds of 200 and 350 cells/μl over a clinically relevant range. The secondary outcome measure was test imprecision, expressed as % coefficient of variation. Thirty-two studies evaluating 15 CD4 technologies were included, of which less than half presented data on bias and misclassification compared to the same reference technology. At CD4 counts <350 cells/μl, bias ranged from -35.2 to +13.1 cells/μl while at counts >350 cells/μl, bias ranged from -70.7 to +47 cells/μl, compared to the BD FACSCount as a reference technology. Misclassification around the threshold of 350 cells/μl ranged from 1-29% for upward classification, resulting in under-treatment, and 7-68% for downward classification resulting in overtreatment. Less than half of these studies reported within laboratory precision or reproducibility of the CD4 values obtained.
Conclusions: A wide range of bias and percent misclassification around treatment thresholds were reported on the CD4 enumeration technologies included in this review, with few studies reporting assay precision. The lack of standardised methodology on test evaluation, including the use of different reference standards, is a barrier to assessing relative assay performance and could hinder the introduction of new point-of-care assays in countries where they are most needed.
Conflict of interest statement
Figures
References
-
- World Health Organization, UNAIDS, UNICEF (2013) Global update on HIV treatment 2013: results, impact and opportunities. Geneva: World Health Organization.
-
- Giorgi JV (1993) Characterization of T lymphocyte subset alterations by flow cytometry in HIV disease. Annals of the New York Academy of Sciences 677: 126–137. - PubMed
-
- Sterling TR, Chaisson RE, Moore RD (2001) HIV-1 RNA, CD4 T-lymphocytes, and clinical response to highly active antiretroviral therapy. Aids 15: 2251–2257. - PubMed
-
- Tayler-Smith K, Zachariah R, Massaquoi M, Manzi M, Pasulani O, et al. (2010) Unacceptable attrition among WHO stages 1 and 2 patients in a hospital-based setting in rural Malawi: can we retain such patients within the general health system? Transactions of the Royal Society of Tropical Medicine and Hygiene 104: 313–319. 10.1016/j.trstmh.2010.01.007 - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
