

A clinical prediction model to identify patients at high risk of death in the emergency department
- PMID: 25792208
- PMCID: PMC4477719
- DOI: 10.1007/s00134-015-3737-x
A clinical prediction model to identify patients at high risk of death in the emergency department
Abstract
Purpose: Rapid assessment and intervention is important for the prognosis of acutely ill patients admitted to the emergency department (ED). The aim of this study was to prospectively develop and validate a model predicting the risk of in-hospital death based on all available information available at the time of ED admission and to compare its discriminative performance with a non-systematic risk estimate by the triaging first health-care provider.
Methods: Prospective cohort analysis based on a multivariable logistic regression for the probability of death.
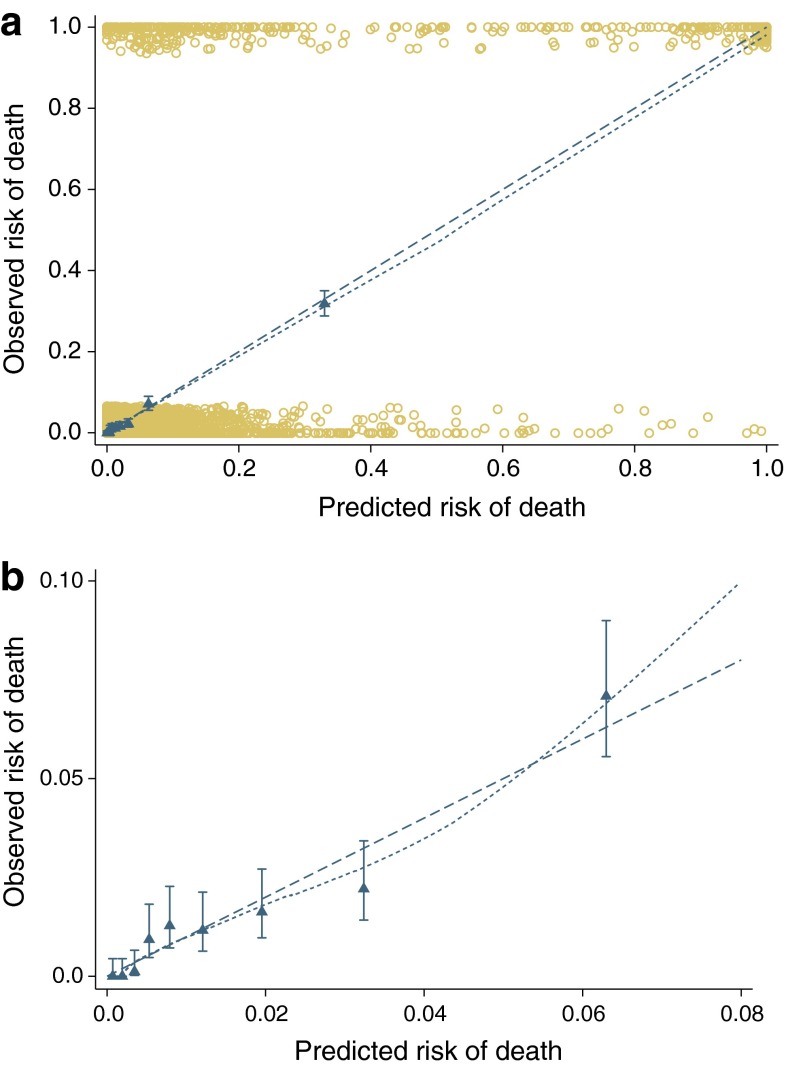
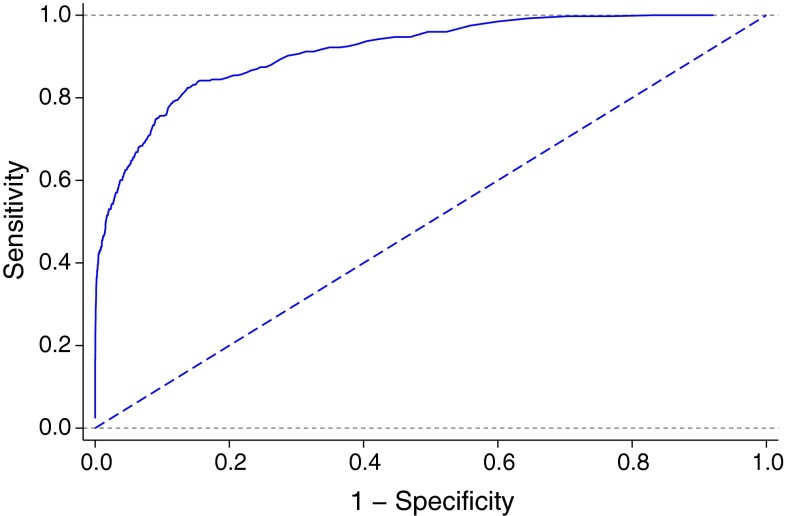
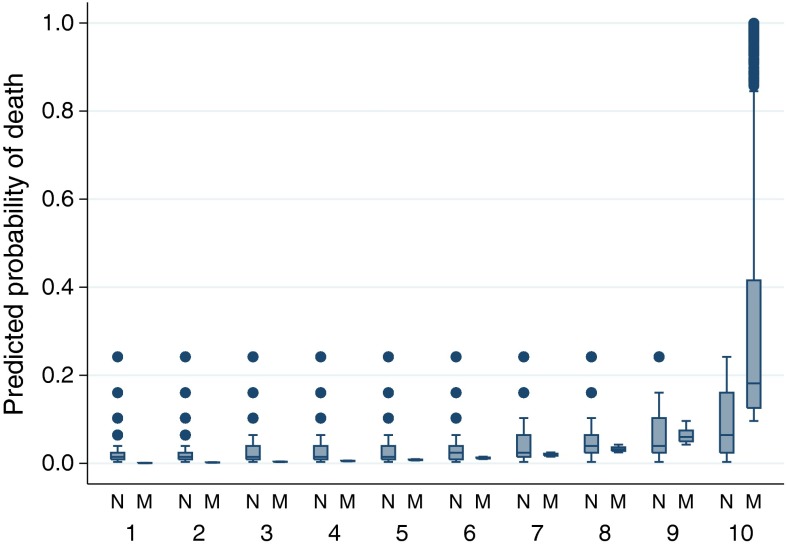
Results: A total of 8,607 consecutive admissions of 7,680 patients admitted to the ED of a tertiary care hospital were analysed. Most frequent APACHE II diagnostic categories at the time of admission were neurological (2,052, 24%), trauma (1,522, 18%), infection categories [1,328, 15%; including sepsis (357, 4.1%), severe sepsis (249, 2.9%), septic shock (27, 0.3%)], cardiovascular (1,022, 12%), gastrointestinal (848, 10%) and respiratory (449, 5%). The predictors of the final model were age, prolonged capillary refill time, blood pressure, mechanical ventilation, oxygen saturation index, Glasgow coma score and APACHE II diagnostic category. The model showed good discriminative ability, with an area under the receiver operating characteristic curve of 0.92 and good internal validity. The model performed significantly better than non-systematic triaging of the patient.
Conclusions: The use of the prediction model can facilitate the identification of ED patients with higher mortality risk. The model performs better than a non-systematic assessment and may facilitate more rapid identification and commencement of treatment of patients at risk of an unfavourable outcome.
Figures
Comment in
-
To score or not to score during triage in the emergency department?Intensive Care Med. 2015 Jun;41(6):1135-7. doi: 10.1007/s00134-015-3814-1. Epub 2015 May 14. Intensive Care Med. 2015. PMID: 25971384 No abstract available.
References
-
- Nguyen HB, Banta JE, Cho TW, Van Ginkel C, Burroughs K, Wittlake WA, Corbett SW. Mortality predictions using current physiologic scoring systems in patients meeting criteria for early goal-directed therapy and the severe sepsis resuscitation bundle. Shock. 2008;30:23–28. doi: 10.1097/SHK.0b013e3181673826. - DOI - PubMed
-
- Kause J, Smith G, Prytherch D, Parr M, Flabouris A, Hillman K. A comparison of antecedents to cardiac arrests, deaths and emergency intensive care admissions in Australia and New Zealand, and the United Kingdom—the ACADEMIA study. Resuscitation. 2004;62:275–282. doi: 10.1016/j.resuscitation.2004.05.016. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
