

Tuberculosis control in South African gold mines: mathematical modeling of a trial of community-wide isoniazid preventive therapy
- PMID: 25792607
- PMCID: PMC4388015
- DOI: 10.1093/aje/kwu320
Tuberculosis control in South African gold mines: mathematical modeling of a trial of community-wide isoniazid preventive therapy
Abstract
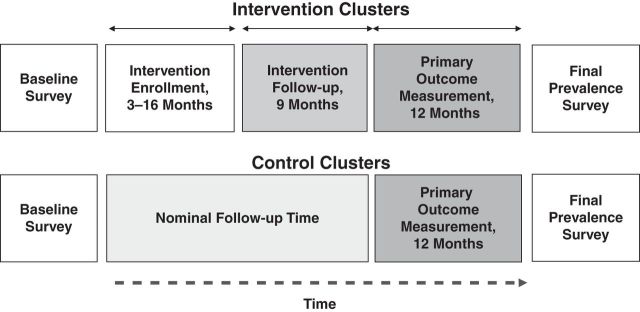
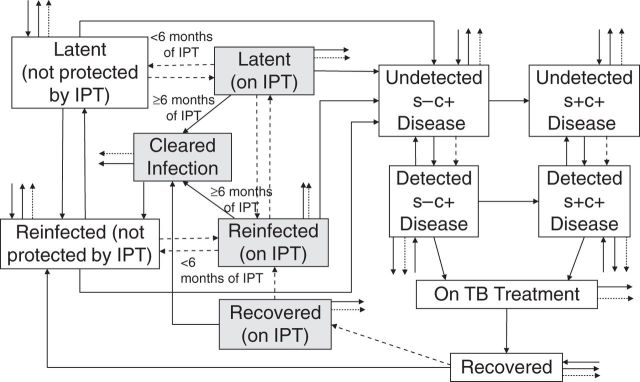
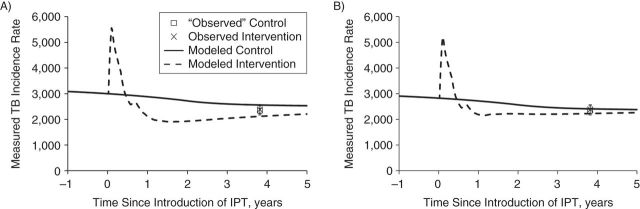
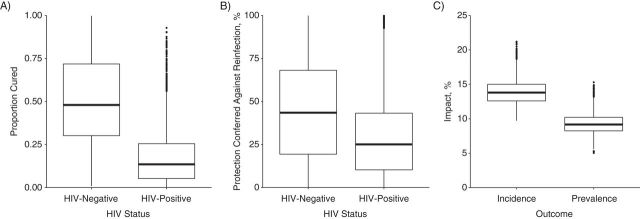
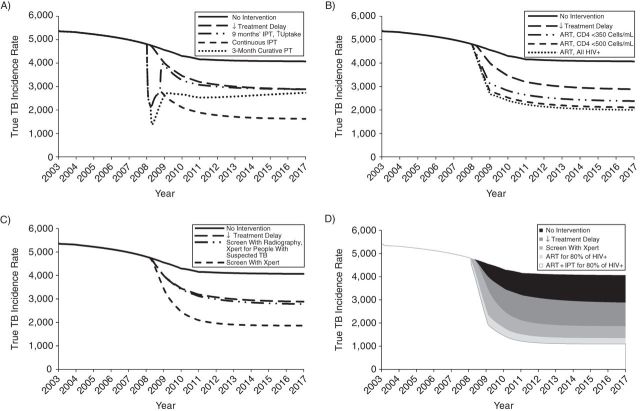
A recent major cluster randomized trial of screening, active disease treatment, and mass isoniazid preventive therapy for 9 months during 2006-2011 among South African gold miners showed reduced individual-level tuberculosis incidence but no detectable population-level impact. We fitted a dynamic mathematical model to trial data and explored 1) factors contributing to the lack of population-level impact, 2) the best-achievable impact if all implementation characteristics were increased to the highest level achieved during the trial ("optimized intervention"), and 3) how tuberculosis might be better controlled with additional interventions (improving diagnostics, reducing treatment delay, providing isoniazid preventive therapy continuously to human immunodeficiency virus-positive people, or scaling up antiretroviral treatment coverage) individually and in combination. We found the following: 1) The model suggests that a small proportion of latent infections among human immunodeficiency virus-positive people were cured, which could have been a key factor explaining the lack of detectable population-level impact. 2) The optimized implementation increased impact by only 10%. 3) Implementing additional interventions individually and in combination led to up to 30% and 75% reductions, respectively, in tuberculosis incidence after 10 years. Tuberculosis control requires a combination prevention approach, including health systems strengthening to minimize treatment delay, improving diagnostics, increased antiretroviral treatment coverage, and effective preventive treatment regimens.
Keywords: mass community-wide isoniazid preventive therapy; mathematical model; tuberculosis.
© The Author 2015. Published by Oxford University Press on behalf of the Johns Hopkins Bloomberg School of Public Health. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Figures
References
-
- World Health Organization. Global Tuberculosis Report, 2012. Geneva, Switzerland: World Health Organization; 2012.
-
- van Halsema CL, Fielding KL, Chihota VN, et al. Trends in drug-resistant tuberculosis in a gold-mining workforce in South Africa, 2002–2008. Int J Tuberc Lung Dis. 2012;167:967–973. - PubMed
-
- Ferebee SH. Controlled chemoprophylaxis trials in tuberculosis. A general review. Bibl Tuberc. 1970;26:28–106. - PubMed
-
- Fielding KL, Grant AD, Hayes RJ, et al. Thibela TB: design and methods of a cluster randomised trial of the effect of community-wide isoniazid preventive therapy on tuberculosis amongst gold miners in South Africa. Contemp Clin Trials. 2011;323:382–392. - PubMed
-
- Churchyard GJ, Fielding KL, Lewis JJ, et al. A trial of mass isoniazid preventive therapy for tuberculosis control. N Engl J Med. 2014;3704:301–310. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
