

Automatic prediction of cardiovascular and cerebrovascular events using heart rate variability analysis
- PMID: 25793605
- PMCID: PMC4368686
- DOI: 10.1371/journal.pone.0118504
Automatic prediction of cardiovascular and cerebrovascular events using heart rate variability analysis
Abstract
Background: There is consensus that Heart Rate Variability is associated with the risk of vascular events. However, Heart Rate Variability predictive value for vascular events is not completely clear. The aim of this study is to develop novel predictive models based on data-mining algorithms to provide an automatic risk stratification tool for hypertensive patients.
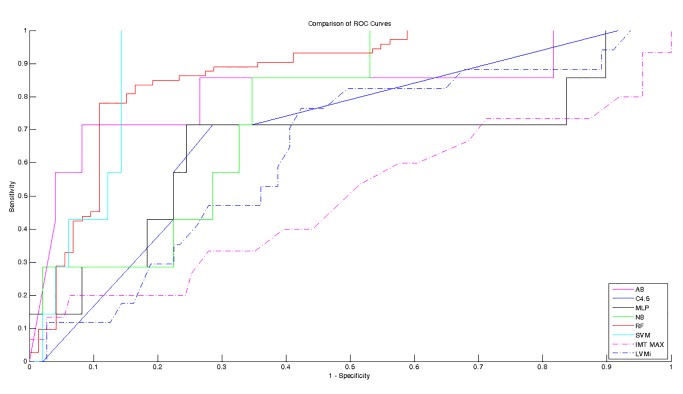
Methods: A database of 139 Holter recordings with clinical data of hypertensive patients followed up for at least 12 months were collected ad hoc. Subjects who experienced a vascular event (i.e., myocardial infarction, stroke, syncopal event) were considered as high-risk subjects. Several data-mining algorithms (such as support vector machine, tree-based classifier, artificial neural network) were used to develop automatic classifiers and their accuracy was tested by assessing the receiver-operator characteristics curve. Moreover, we tested the echographic parameters, which have been showed as powerful predictors of future vascular events.
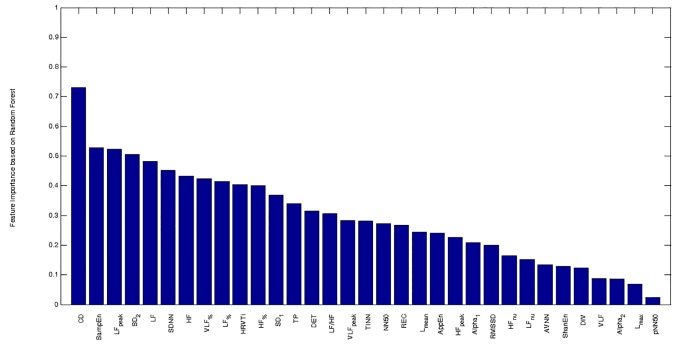
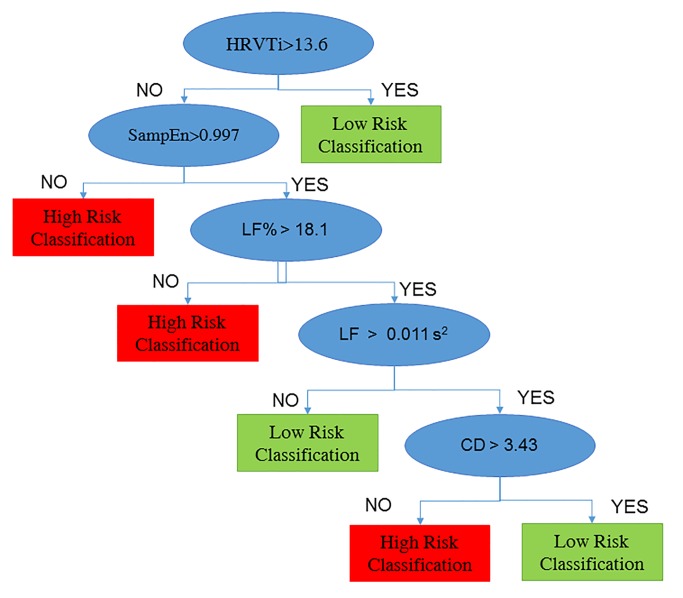
Results: The best predictive model was based on random forest and enabled to identify high-risk hypertensive patients with sensitivity and specificity rates of 71.4% and 87.8%, respectively. The Heart Rate Variability based classifier showed higher predictive values than the conventional echographic parameters, which are considered as significant cardiovascular risk factors.
Conclusions: Combination of Heart Rate Variability measures, analyzed with data-mining algorithm, could be a reliable tool for identifying hypertensive patients at high risk to develop future vascular events.
Conflict of interest statement
Figures
References
-
- Fuster V. Epidemic of cardiovascular disease and stroke: the three main challenges. Presented at the 71st scientific sessions of the American Heart Association. Dallas, Texas. Circulation. 1999;99(9):1132–7. PubMed PMID: . - PubMed
-
- Rothwell PM, Coull AJ, Silver LE, Fairhead JF, Giles MF, Lovelock CE, et al. Population-based study of event-rate, incidence, case fatality, and mortality for all acute vascular events in all arterial territories (Oxford Vascular Study). Lancet. 2005;366(9499):1773–83. 10.1016/S0140-6736(05)67702-1 PubMed PMID: . - DOI - PubMed
-
- Nagai K, Shibata S, Akishita M, Sudoh N, Obara T, Toba K, et al. Efficacy of combined use of three non-invasive atherosclerosis tests to predict vascular events in the elderly; carotid intima-media thickness, flow-mediated dilation of brachial artery and pulse wave velocity. Atherosclerosis. 2013;231(2):365–70. 10.1016/j.atherosclerosis.2013.09.028 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
