

Occipital nerve stimulation for chronic migraine--a systematic review and meta-analysis
- PMID: 25793740
- PMCID: PMC4368787
- DOI: 10.1371/journal.pone.0116786
Occipital nerve stimulation for chronic migraine--a systematic review and meta-analysis
Abstract
Background: Chronic migraine is a debilitating headache disorder that has significant impact on quality of life. Stimulation of peripheral nerves is increasingly being used to treat chronic refractory pain including headache disorders. This systematic review examines the effectiveness and adverse effects of occipital nerve stimulation (ONS) for chronic migraine.
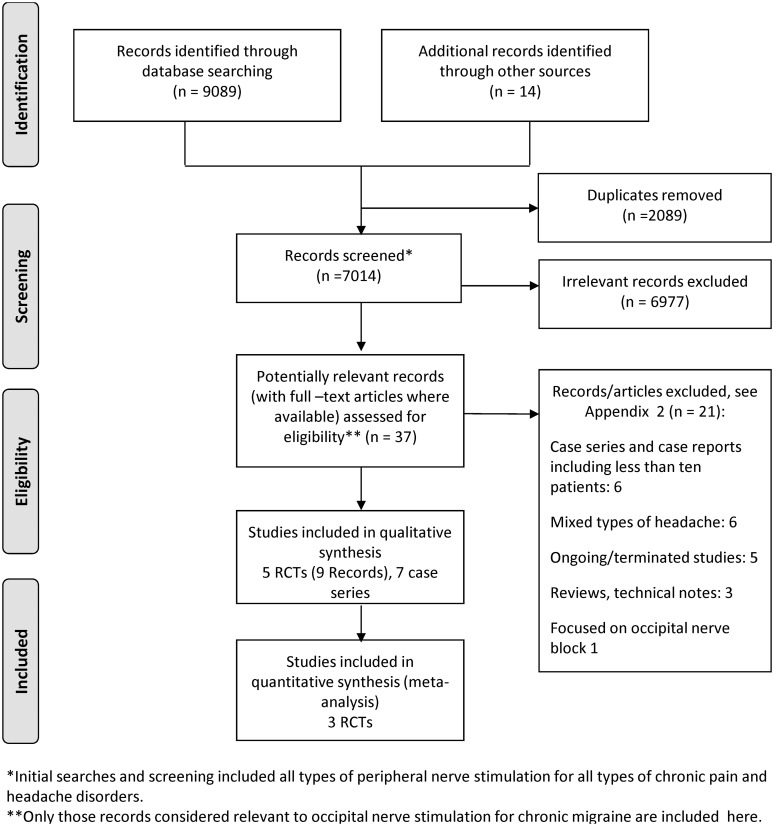
Methods: Databases, including the Cochrane Library, MEDLINE, EMBASE, CINAHL and clinical trial registers were searched to September 2014. Randomized controlled trials (RCTs), other controlled and uncontrolled observational studies and case series (n≥ 10) were eligible. RCTs were assessed using the Cochrane risk of bias tool. Meta-analysis was carried out using a random-effects model. Findings are presented in summary tables and forest plots.
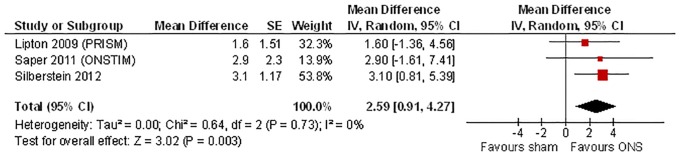
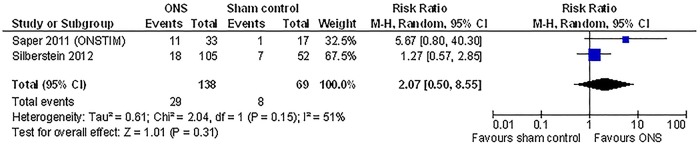
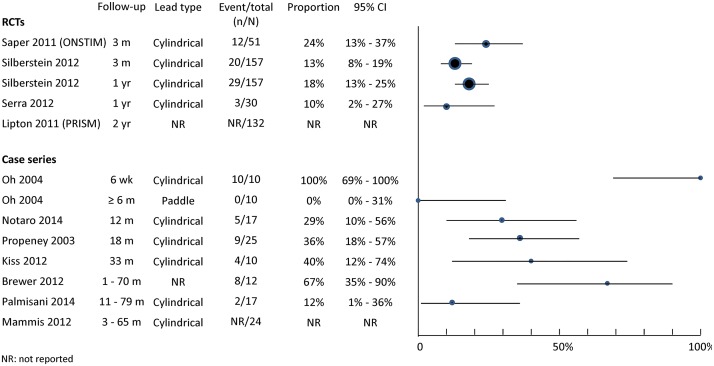
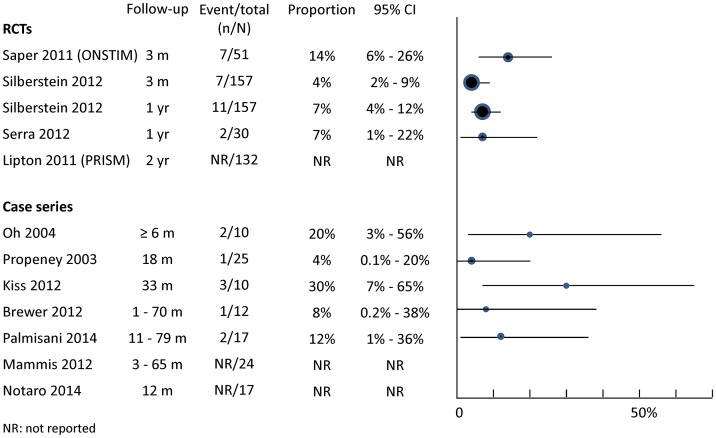
Results: Five RCTs (total n=402) and seven case series (total n=115) met the inclusion criteria. Pooled results from three multicenter RCTs show that ONS was associated with a mean reduction of 2.59 days (95% CI 0.91 to 4.27, I2=0%) of prolonged, moderate to severe headache per month at 3 months compared with a sham control. Results for other outcomes generally favour ONS over sham controls but quantitative analysis was hampered by incomplete publication and reporting of trial data. Lead migration and infections are common and often require revision surgery. Open-label follow-up of RCTs and case series suggest long-term effectiveness can be maintained in some patients but evidence is limited.
Conclusions: While the effectiveness of ONS compared to sham control has been shown in multiple RCTs, the average effect size is modest and may be exaggerated by bias as achieving effective blinding remains a methodological challenge. Further measures to reduce the risk of adverse events and revision surgery are needed.
Systematic review registration: this systematic review is an update and expanded work of part of a broader review registered with PROSPERO. Registration No. CRD42012002633.
Conflict of interest statement
Figures
References
-
- Vos T, Flaxman AD, Naghavi M, Lozano R, Michaud C, et al. (2012) Years lived with disability (YLDs) for 1160 sequelae of 289 diseases and injuries 1990–2010: a systematic analysis for the Global Burden of Disease Study 2010. The Lancet 380: 2163–2196. 10.1016/S0140-6736(12)61729-2 - DOI - PMC - PubMed
-
- Silberstein SD, Lipton RB, Solomon S, Mathew NT (1994) Classification of daily and near-daily headaches: proposed revisions to the IHS criteria. Headache 34: 1–7. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
