

Cost-effectiveness of adding bedaquiline to drug regimens for the treatment of multidrug-resistant tuberculosis in the UK
- PMID: 25794045
- PMCID: PMC4368676
- DOI: 10.1371/journal.pone.0120763
Cost-effectiveness of adding bedaquiline to drug regimens for the treatment of multidrug-resistant tuberculosis in the UK
Abstract
Objective: To evaluate the cost-effectiveness of adding bedaquiline to a background regimen (BR) of drugs for multidrug-resistant tuberculosis (MDR-TB) in the United Kingdom (UK).
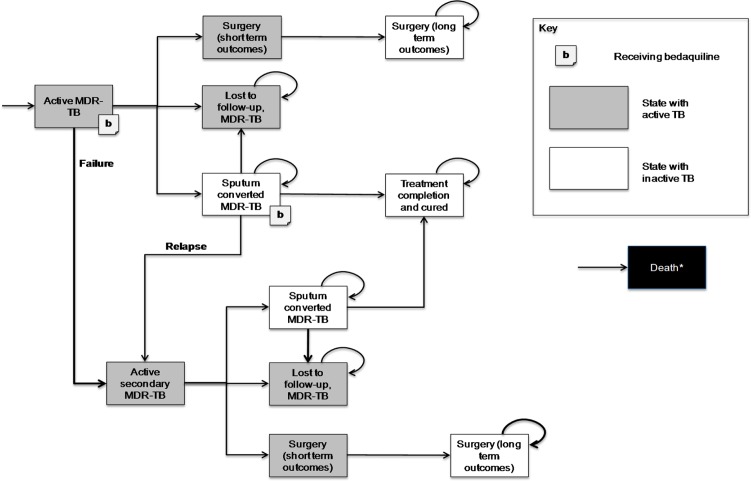
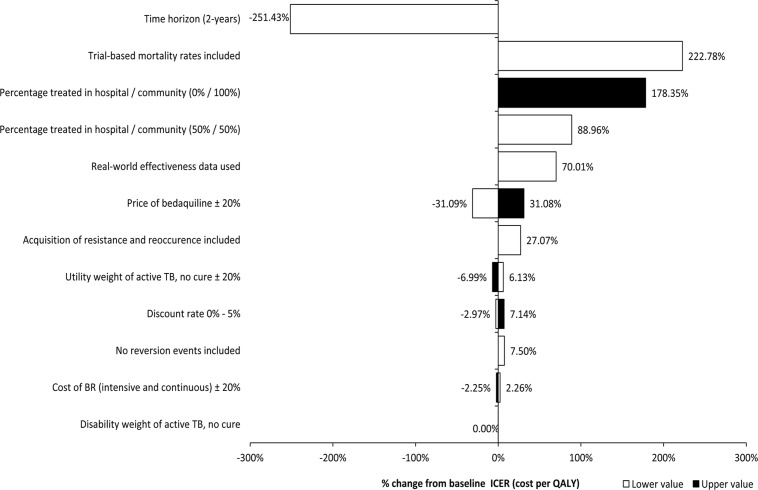
Methods: A cohort-based Markov model was developed to estimate the incremental cost-effectiveness ratio of bedaquiline plus BR (BBR) versus BR alone (BR) in the treatment of MDR-TB, over a 10-year time horizon. A National Health Service (NHS) and personal social services perspective was considered. Cost-effectiveness was evaluated in terms of Quality-Adjusted Life Years (QALYs) and Disability-Adjusted Life Years (DALYs). Data were sourced from a phase II, placebo-controlled trial, NHS reference costs, and the literature; the US list price of bedaquiline was used and converted to pounds (£18,800). Costs and effectiveness were discounted at a rate of 3.5% per annum. Probabilistic and deterministic sensitivity analysis was conducted.
Results: The total discounted cost per patient (pp) on BBR was £106,487, compared with £117,922 for BR. The total discounted QALYs pp were 5.16 for BBR and 4.01 for BR. The addition of bedaquiline to a BR resulted in a cost-saving of £11,434 and an additional 1.14 QALYs pp over a 10-year period, and is therefore considered to be the dominant (less costly and more effective) strategy over BR. BBR remained dominant in the majority of sensitivity analyses, with a 81% probability of being dominant versus BR in the probabilistic analysis.
Conclusions: In the UK, bedaquiline is likely to be cost-effective and cost-saving, compared with the current MDR-TB standard of care under a range of scenarios. Cost-savings over a 10-year period were realized from reductions in length of hospitalization, which offset the bedaquiline drug costs. The cost-benefit conclusions held after several sensitivity analyses, thus validating assumptions made, and suggesting that the results would hold even if the actual price of bedaquiline in the UK were higher than in the US.
Conflict of interest statement
Figures


References
-
- WHO. Tuberculosis Fact Sheet Number 104. October 2014. Available: http://www.who.int/mediacentre/factsheets/fs104/en/index.html. Accessed 2015 Feb 12.
-
- HPA. Tuberculosis in the UK: 2013 report. January 2014. Available: https://www.gov.uk/government/uploads/system/uploads/attachment_data/fil.... Accessed 2015 Feb 12.
-
- ECDC. Tuberculosis surveillance and monitoring in Europe. 2013. Available: http://www.ecdc.europa.eu/en/publications/Publications/Tuberculosis-surv.... Accessed 2015 Feb 12.
-
- Curry International TB Center. CITC (Curry International Tuberculosis Center) and TBCB (TB control branch) of California department, Drug-resistant tuberculosis: a survival guide for clinicians. 2008.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
