

Effect of cytomegalovirus co-infection on normalization of selected T-cell subsets in children with perinatally acquired HIV infection treated with combination antiretroviral therapy
- PMID: 25794163
- PMCID: PMC4368806
- DOI: 10.1371/journal.pone.0120474
Effect of cytomegalovirus co-infection on normalization of selected T-cell subsets in children with perinatally acquired HIV infection treated with combination antiretroviral therapy
Abstract
Background: We examined the effect of cytomegalovirus (CMV) co-infection and viremia on reconstitution of selected CD4+ and CD8+ T-cell subsets in perinatally HIV-infected (PHIV+) children ≥ 1-year old who participated in a partially randomized, open-label, 96-week combination antiretroviral therapy (cART)-algorithm study.
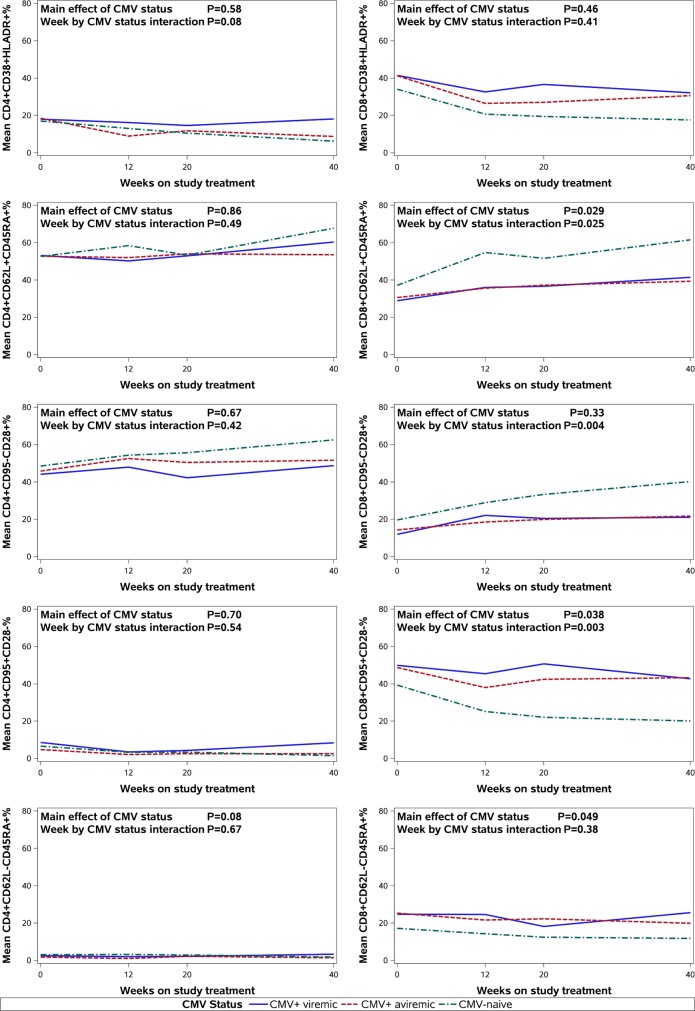
Methods: Participants were categorized as CMV-naïve, CMV-positive (CMV+) viremic, and CMV+ aviremic, based on blood, urine, or throat culture, CMV IgG and DNA polymerase chain reaction measured at baseline. At weeks 0, 12, 20 and 40, T-cell subsets including naïve (CD62L+CD45RA+; CD95-CD28+), activated (CD38+HLA-DR+) and terminally differentiated (CD62L-CD45RA+; CD95+CD28-) CD4+ and CD8+ T-cells were measured by flow cytometry.
Results: Of the 107 participants included in the analysis, 14% were CMV+ viremic; 49% CMV+ aviremic; 37% CMV-naïve. In longitudinal adjusted models, compared with CMV+ status, baseline CMV-naïve status was significantly associated with faster recovery of CD8+CD62L+CD45RA+% and CD8+CD95-CD28+% and faster decrease of CD8+CD95+CD28-%, independent of HIV VL response to treatment, cART regimen and baseline CD4%. Surprisingly, CMV status did not have a significant impact on longitudinal trends in CD8+CD38+HLA-DR+%. CMV status did not have a significant impact on any CD4+ T-cell subsets.
Conclusions: In this cohort of PHIV+ children, the normalization of naïve and terminally differentiated CD8+ T-cell subsets in response to cART was detrimentally affected by the presence of CMV co-infection. These findings may have implications for adjunctive treatment strategies targeting CMV co-infection in PHIV+ children, especially those that are now adults or reaching young adulthood and may have accelerated immunologic aging, increased opportunistic infections and aging diseases of the immune system.
Conflict of interest statement
Figures

References
-
- UNAIDS Global Report 2013. Available: http://www.unaids.org/en/resources/infographics/20131120aidsbythenumbers02/ Accessed 24 June, 2014.
-
- Rosenblatt HM, Stanley KE, Song LY, Johnson GM, Wiznia AA, Nachman SA et al. Immunological response to highly active antiretroviral therapy in children with clinically stable HIV-1 infection. J Infect Dis. 2005;192: 445–455. - PubMed
-
- Appay V, Sauce D. Immune activation and inflammation in HIV-1 infection: causes and consequences. J Pathol. 2008;214: 231–241. - PubMed
-
- Kovacs A, Schluchter M, Easley K, Demmler G, Shearer W, La Russa P, et al. Cytomegalovirus infection and HIV-1 disease progression in infants born to HIV-1-infected women. Pediatric Pulmonary and Cardiovascular Complications of Vertically Transmitted HIV Infection Study Group N Engl J Med. 1999;341: 77–84. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
