

Magnetic resonance imaging of sellar and juxtasellar abnormalities in the paediatric population: an imaging review
- PMID: 25794595
- PMCID: PMC4376809
- DOI: 10.1007/s13244-015-0401-5
Magnetic resonance imaging of sellar and juxtasellar abnormalities in the paediatric population: an imaging review
Abstract
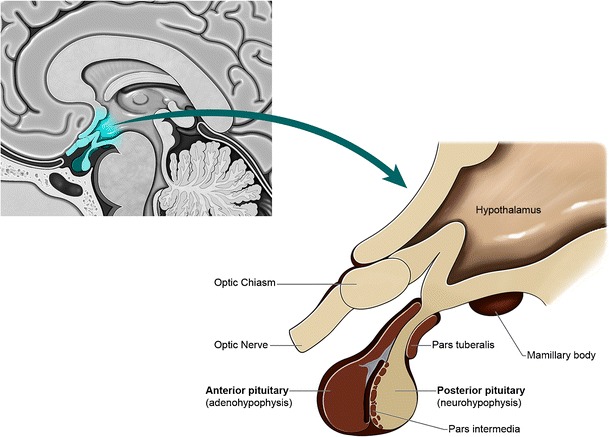
The sellar and juxtasellar regions in the paediatric population are complex both anatomically and pathologically, with magnetic resonance imaging (MRI) being the "gold standard" imaging modality due to the high contrast of detail. Assessment requires a detailed understanding of the anatomy, embryology, pathophysiology and normal signal characteristics of the pituitary gland and surrounding structures in order to appropriately characterise abnormalities. This article aims to provide an overview of the imaging characteristics of developmental/congenital and acquired disease processes which affect the sellar and juxtasellar region in the paediatric population. Main Messages • The sellar region is anatomically complex and covers a wide pathology spectrum. • MRI is the key imaging modality to assess sellar and juxtasellar pathology. • Numerous developmental anomalies may not be discovered until adulthood. • Knowledge of pathology alerts and guides the clinician towards appropriate management.
Figures




























References
-
- Fujisawa I, Asato R, Nishimura K et al (1987) Anterior and posterior lobes of the pituitary gland: assessment by 1.5 T MR imaging. J Comput Assist Tomogr 11:214–220 - PubMed
-
- Nishimura K, Fujisawa I, Togashi K et al (1986) Posterior lobe of the pituitary: identification by lack of chemical shift artifact in MR imaging. J Comput Assist Tomogr 10:899–902 - PubMed
-
- Fujisawa I, Asato R, Kawata M et al (1989) Hyperintense signal of the posterior pituitary on T1-weighted MR images: an experimental study. J Comput Assist Tomogr 13:371–377 - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
